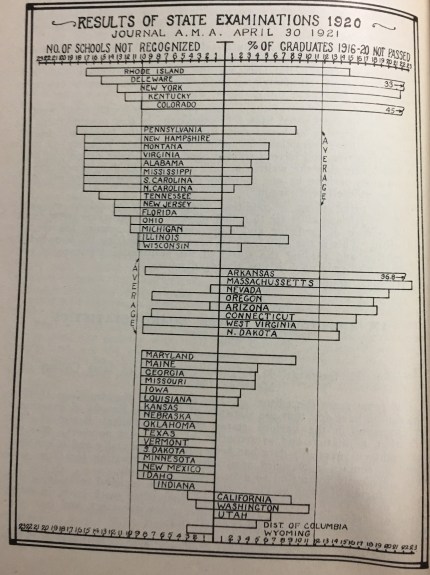
Last time I explained the authority of state medical boards to identify “approved” and “unapproved” medical schools as one criteria in the decision to issue or deny a medical license—one of the “lost” powers of state medical boards. The information presented on the left side of the chart below reflects this information.[1] Now let’s explore the other side of the chart.
Co-existing with the statutory authority of state boards to issue a license for the practice of medicine is their primary historical function—developing and administering an exam to determine the knowledge of a prospective licensee.
As noted earlier, the quality of U.S. medical schools varied widely in the late 19th and early 20th centuries. Thus, the medical degree could not be accepted at face value as definitive evidence of preparedness to practice medicine. Accordingly, state medical boards were empowered to independently assess the knowledge of prospective licensees.
State medical boards—or the state board of medical examiners to use the more common title of that era—embraced this assessment role. Their exams typically were multi-day affairs relying upon open-ended questions, i.e., extended short answer or essay questions.
Look closely at the right side of this chart; one element jumps out immediately. The fail rate on these exams differed dramatically among the various states. At one end of the spectrum, sixteen states reported a fail rate of less than 1% on their licensing examination over the period from 1916-1920.
At first, I was suspicious whether this was accurate so I double checked the JAMA state board issues for this period. Sure enough, in places like Vermont and Idaho only 1-2 people failed during this entire period. Thus, a fail rate of less than 1% was accurate.
At the other end of this spectrum, five states reported fail rates of 22% or higher during this period. These weren’t all small states either. Heavily populated states like Massachusetts and Pennsylvania were in this cohort.
Furthermore, there didn’t seem to be a strong correlation between the number of schools not recognized by a state and the fail rate on its exam. Theoretically, we’d expect states like Delaware and Massachusetts to have lower fail rates because they already precluded so many graduates from substandard schools from sitting their exam. Yet, their fail rates were actually quite high—33% and 23% respectively.
Similarly, we might anticipate a higher fail rate in places like Utah and the District of Columbia since they precluded no one from sitting their exam. Yet, their fail rates were modest (5-7%) and well below the national average.
All of which leads to a suspicion that state medical board exams of this era were idiosyncratic tools that diverged markedly not only in their rigor (i.e., pass/fail standard) but probably to some extent in their content as well.
![]() It is no wonder that the National Board of Medical Examiners developed and administered a certifying exam beginning in 1916 with eligibility criteria and professional standards designed to meet and exceed those of every state board exam…and no wonder that thirty-one states by 1925 accepted a pass on this exam as meeting their requirements for licensure.[2]
It is no wonder that the National Board of Medical Examiners developed and administered a certifying exam beginning in 1916 with eligibility criteria and professional standards designed to meet and exceed those of every state board exam…and no wonder that thirty-one states by 1925 accepted a pass on this exam as meeting their requirements for licensure.[2]
State medical boards remained in the business of creating licensing examinations until the late 1960s when the transition to nationally developed exams began. I’ll talk about that transition later.
Technically, state medical boards have not “lost” the power of assessment. What has happened is a shift in statutory language reflecting these boards’ responsibility to identify the examination(s) they will recognize and accept as evidence of medical knowledge: USMLE and COMLEX-USA.
![]()
They have delegated (wisely) the daunting task of developing and administering their own medical licensing exam to professional entities with expertise in the science of assessment. In doing so, these boards retain their key role as an invaluable independent audit of medical education with their exam…but now they do so in concert with experts in assessment.
The opinions expressed are those of the author and not the FSMB.
[1] Federation Bulletin, June 1921, p.
[2] Johnson, Chaudhry. Medical Licensing and Discipline in America, 72.
