It would be naïve to think that this nation’s fraught history with race did not impact medical regulation. The challenge here, as for all the categories explored in this post, is pulling together a reasonable overarching narrative from fifty different states. If we pull back to a thirty-thousand foot view for medical regulation, however, there was one development that carried by far the greatest impact.
Black Americans faced limited opportunities for medical education and, ultimately, licensure in the late 19th and early 20th century. These opportunities were curtailed further by reform measures in medical education such as those by the Carnegie Foundation and the AMA Council on Medical Education. While the Carnegie Foundation’s Flexner Report remains the better known of these efforts, the Council on Medical Education’s inspection and rating system for U.S. medical schools proved even more impactful. You may wonder, “How is this relevant to medical regulation?” I’ll explain.
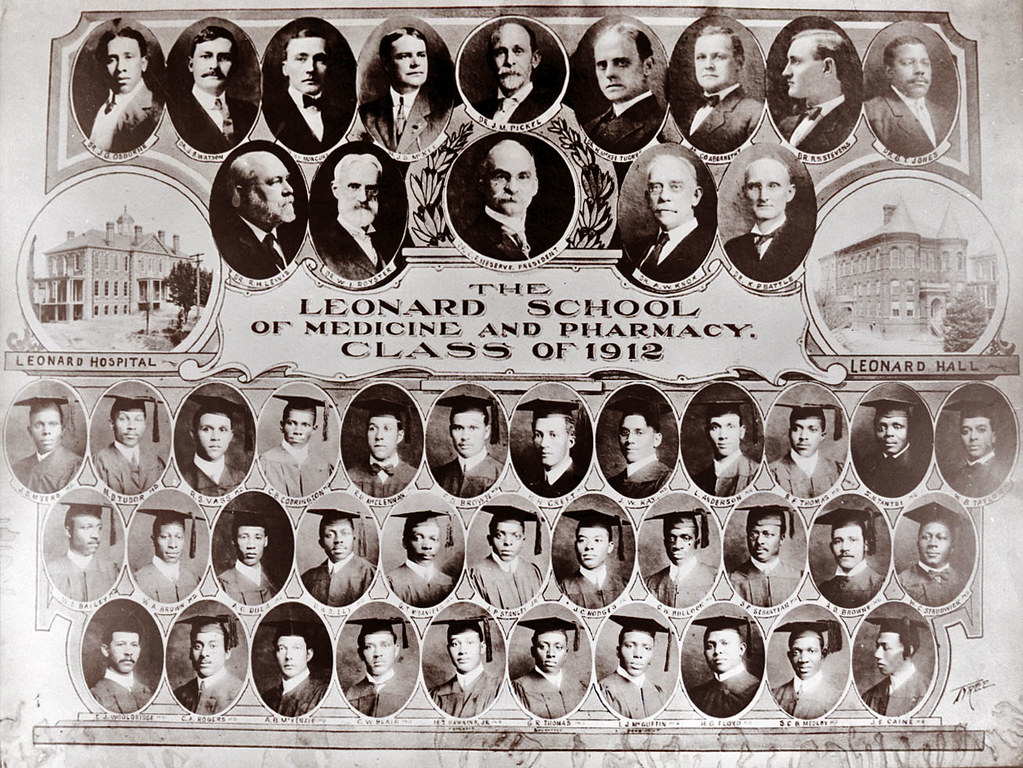
The Council created a 3-tier rating system that categorized all schools as Class A, Class B or Class C. The first two categories either met standards or were deemed capable of doing so with reasonable changes. Class C schools were classified as substandard and deemed unsalvageable. This categorization system carried a profoundly negative impact to historically black medical colleges (HBMCs), nearly all of which fell into the Class C grouping.
With the exception of Howard, HBMCs were proprietary endeavors chronically short on funding and resources. Yet they were often the only option available to black physician hopefuls. As state legislatures and medical boards –desirous of higher standards for medical education and plagued by persistent diploma mill style educational endeavors—eagerly embraced the Council’s rating system. The classification system fit conveniently and without ambiguity into state law and seemed a mom-n-apple pie recipe for improving the quality of this nation’s physicians.
The downside? Once this became a primary basis for licensure, HBMCs routinely found themselves assigned to the Class C category with their graduates’ ineligible for licensure in all but a few states by 1923. This reality contributed to a death spiral for all but two HBMCs (Howard, Meharry) and represented a massive setback for black Americans aspiring to become licensed physicians.
While this systemic factor cannot be emphasized too much, there was also impactful activity happening around licensing decisions specific to individual physicians. Here it is difficult to generalize without succumbing to speculation. So I will offer a few anecdotes though I acknowledge that the plural of anecdote is not evidence!
Justina Ford was the first black female physician licensed in Colorado. The year was 1902. Her encounter with the Colorado board left an indelible memory. As she related the story later, one board member told her: “I’d feel dishonest taking a [licensing] fee from you. You’ve got two strikes against you. First off, you’re a lady and second, you’re colored.” Her low-key response suggested she would be a persistent licensure applicant. “I know it. I thought it all through before I came. This is just the place I want to practice.”

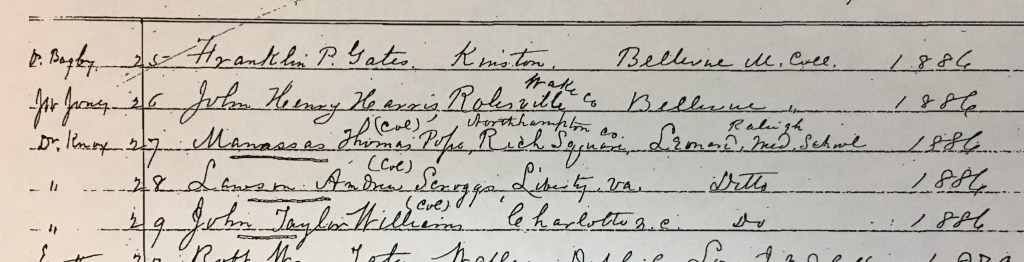
Or take the example of the North Carolina Medical Board. For roughly 40 years, the Board’s administrative practice was to annotate the record of black licensure applicants with a “col” or “colored.” I wrote about this practice recently in the North Carolina Historical Review though the extant evidence and data available were ambiguous as to whether this impacted the scoring of their examination.
It seems highly unlikely that North Carolina was the only state medical board utilizing this annotation practice. It was common to see state medical journals and JAMA publishing updates from medical boards on the administration of their licensing exam…and also common for these narrative pieces to call out the number and/or performance of “colored” candidates. Clearly, someone at these boards was keeping track; and in an era when extended response/essay questions were the norm…well, scoring these licensing exam questions was inherently a subjective matter by the board member(s). Scorer bias—whether racial or subject-matter specific—was impossible to remove from such a testing format.
The Journal of the National Medical Association commented in 1910 on the challenge confronting black physicians to receive due and appropriate credit for their performance on state licensing examinations. Historian Neil McMillian asserted that it was “an article of faith” among black physician candidates in Mississippi that prejudice impacted licensing decisions in that state. The truth behind these concerns and perceptions—to the extent it is recoverable at all—is buried in records dispersed across fifty states. Records that may be suggestive but not explicit about this reality.
Final thoughts
I know that some readers will react to a blog entry like this and think I’m picking at an old wound…that I’m focusing unnecessarily on past shortcomings rather than celebrating the more recent successes in the regulatory narrative. I guess that is one way to interpret this post.
I would hope, however, that readers of this blog over the past few years will see this piece for what I intended—to share what I suspect is a lesser-known aspect of the history of medical regulation; to tell stories—both good and bad—about this unique field; and to inform today’s regulators about the rich history in their field as helpful context for the important work they do today.
Select sources:
Federation Bulletin spanning multiple years from 1915-1926.
“State Board Statistics” in JAMA. This extensive presentation of aggregated information/data appeared annually in April-May.
Marilyn Griggs Riley, High Altitude Attitudes: Six Savvy Colorado Women (Boulder: Johnson Books, 2006)
David Alan Johnson, “The North Carolina Medical Licensing Examination, 1886-1925: Analysis of Performance by Examinees from Historically Black Medical Colleges,” The North Carolina Historical Review (April 2021).
The opinions expressed are those of the author and do not represent the views of his employer (Federation of State Medical Boards)