I’ve debated how I wanted to begin this post. I finally decided to open with the two pictures you see below. Both show the governing board for the Federation of State Medical Boards, the national organization supporting medical licensing authorities throughout the U.S. On the left is the board in 1960; on the right, the current board. The two photos offer a striking contrast and they are also representative of this board’s composition—and that of medical regulation generally—in their respective eras.


Looking at these photos, it’s tempting to craft a soothing narrative, one allowing us to pat ourselves on the back and feel good about the progress we’ve made. Some might say: “Why shouldn’t we?” The visual evidence of progress in terms of diversity is obvious and worth celebrating. Yes, absolutely. Still…contenting ourselves with just that story tends to gloss over the harsher features in the long history of medical regulation, including systemic factors that may still be relevant.
Let’s start with what I think is a key to understanding this history: Medical regulation justified its creation as serving the interests of the public; yet for most of its history, this regulatory framework reflected the demographics, interests and priorities of the medical profession, just as much, if not more than, those of the public.
Medicine as a profession has enjoyed significant latitude in policing itself, i.e., “self-regulating.” While the self-regulatory aspect of medicine today is far less pronounced than it once was, the long historical record, including the late nineteenth century creation of state-based licensing, reflects a clear self-regulatory model. This means that any bias and discriminatory elements in the profession tended to flow inexorably into medical regulation as well. How so? Let’s start with gender.
Women
From an historical perspective, medicine as a field has not been especially inviting of women. Similarly, positions of authority within the field were few and far between for women until more recent decades. Consequently, women were absent from medical boards throughout most of their history.
Granted, we can find the unusual historical first (Dr. Adele Hutchinson appointed to the Minnesota board in 1899) but otherwise the best evidence suggests medical regulation saw few women participating until the 1980s. For example, consider just a cursory breakdown by gender of medical board members between 1985 and 2018. Women comprised only 16% of all board members in 1985. Even that figure is arguably misleading as there were 17 boards with no women serving at all at that time. In 2018, the figure rose to 33% for women serving on state medical boards.

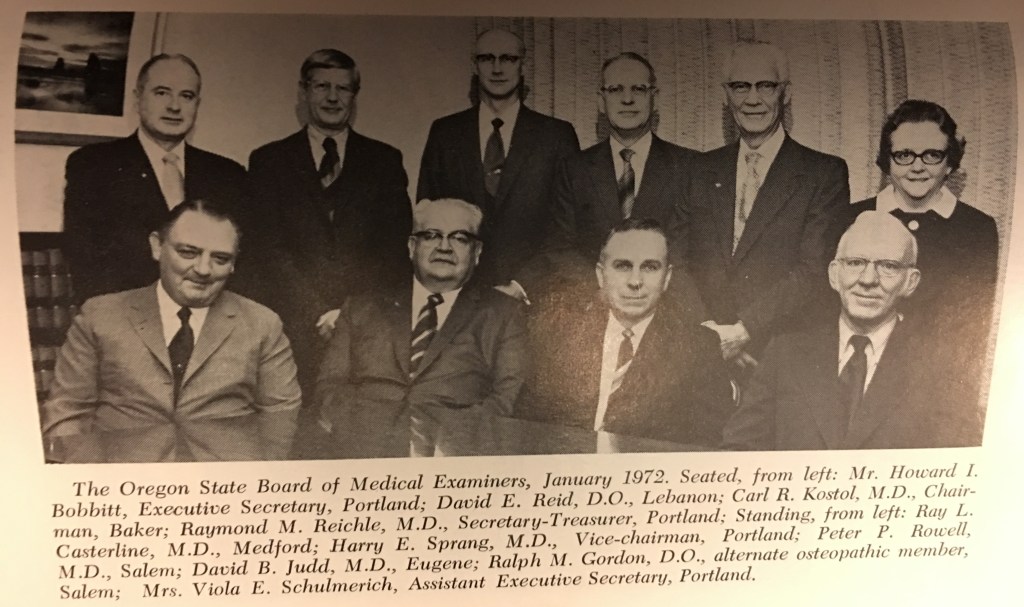
And what of the long period preceding this? Absent a historical listing of all state medical board rosters, it is impossible to offer a definitive statement characterizing the gender landscape for medical regulation between Adele Hutchinson and the mid-1980s. However, there is suggestive photographic evidence. The Federation Bulletin—a monthly FSMB journal—published group photos of medical boards on a periodic basis between 1956 and 1984. A visual review shows that the Bulletin published 29 such photos showing 254 people—only 6 were women. While the available evidence is admittedly limited, it seems sufficient to safely state medical regulation remained male-dominated until recent decades.
Systemic Factor
I know that some will greet my assertion of an historically male-dominated medical regulatory system with a collective, “Duh!” Sheer numbers were one factor. The number of female physicians in this country hovered around seven to eight thousand from about 1900 to 1940. Yet numbers alone don’t tell the story. Instead, it is important to recall the mechanism by which individuals made their way onto state medical boards.
In almost all instances, state medical board members were (and remain today) gubernatorial appointments. In some instances, unilaterally appointed though often with input from the profession via the state medical association. Gender and racial norms throughout the first half of the 20th century differed significantly from today. At a time when Jim Crow segregation predominated in much of the country and women were still fighting for a Constitutional right to vote (1920), the power dynamics in medicine—and thus medical regulation—were slanted almost entirely toward white, male physicians. In essence, even if women or persons of color wished to serve on a state medical board, the likelihood of their doing so was slim at best simply due to the power dynamics at work.
This is an important point that should not be glossed over. Access to power—often predicated upon proximity to, or personal acquaintance with, persons already in a position of power or influence—remains important even today. Talk to individuals appointed to a state medical board today and two themes often crop up as they relate how they came to be appointed. Their stories usually involve either (1) a personal relationship with someone in a position of authority/influence—sometimes even the governor him/herself, or (2) prior direct political engagement or activism bringing the person into contact with key figures in the decision-making dynamics. Whatever the collective composition of state medical boards today (and none of us know precisely what it is), it is undoubtedly much more representative than its past iterations. But it is also still impacted by the dynamics of power and access to that power.
In part two of this blog series, we will consider the regulatory experience of two more groups—international medical graduates (IMGs) and osteopathic physicians. A century ago regulators targeted both groups with measures intended marginalize and limit their ability to practice medicine.
The opinions expressed are those of the author and do not represent the views of his employer (Federation of State Medical Boards)
