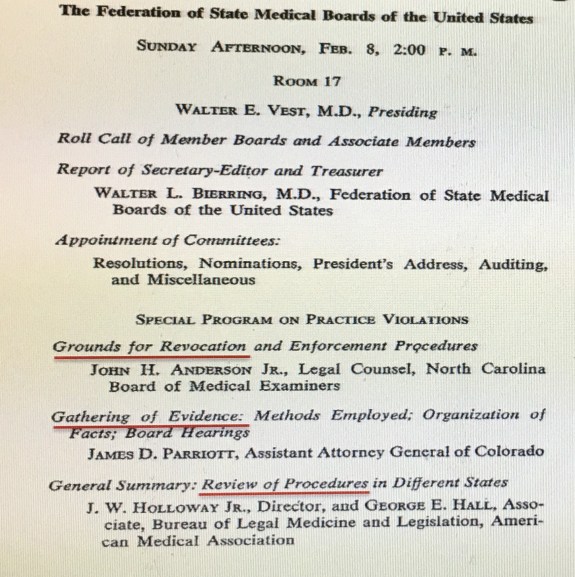
In my last blog entry, I shared the page (below right) from the 1953 FSMB annual meeting program. I did so in order to spotlight the fact that discipline was such a minor concern of state medical boards that as a topic it appeared only once (1953) on the formal program of the Federation’s annual meeting during the decade of the Fifties.
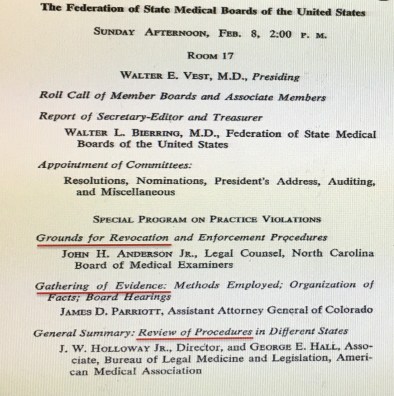
I think any member of a state medical board or its staff looking at this today would find this remarkable. After all, they understand all too well the extent to which the disciplinary role is a time, labor and resource intensive element of medical boards’ functioning.
So what was going on during the 1950s? Certainly physicians in those days were not demi-gods immune to human flaws and failures. I think a couple factors were at work.
Medical boards of that era still thought largely in terms of the primary function envisioned for them at the time of their creation in the late 19th century—writing and developing an examination to assess physician knowledge prior to issuing a medical license.
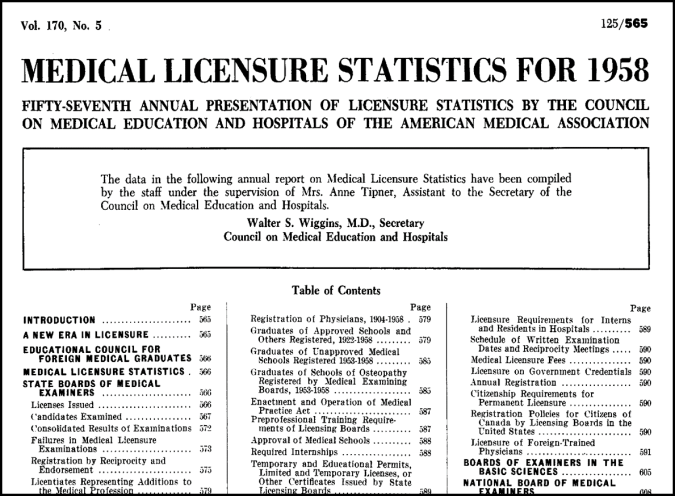
Just how much priority and precedence did this aspect of medical boards’ activities take? It would be difficult to overstate the case. Take this example. From 1906 to the mid-1960s, JAMA produced an annual issue featuring statistical data on the medical licensing examinations each year. (example below) Examinee counts, pass rates, licenses issued, statistical breakdowns by board, by medical school, etc. The list could go on for several paragraphs but my point is simple. Administering examinations and issuing licenses were the heart-n-soul of medical board activities in the 1950s. That is where they placed their greatest emphasis and focus.
So what does this mean about discipline? Here I will offer the opinions of a few medical regulators of the day. Asked about the disciplinary role of state medical boards in 1952, the FSMB’s own president said, “The influence of professional organizations coupled with the desire for the respect of fellow practitioners is usually sufficient.” One regulator, when asked about his board’s budget for disciplinary investigations, explained that “none is needed” because “discipline is…of secondary importance.”
Admittedly, the plural of anecdote is not evidence. Yet statements like these from medical regulators of that era seem telling.
This is not to say that state medical boards had abandoned their disciplinary role entirely. While no definitive national data exists for this period, my own count of disciplinary actions published through the Federation Bulletin found approximately 1,800 actions taken by boards between 1950 and 1959. To put that in at least some type of context, in 2015 medical boards in the U.S. took 7,000 actions that year alone.
Ultimately, the problem of discipline in that era was attitudinal. The regulators themselves did not see discipline as a priority; in part, because they presumed others were tending to this. Specifically, the literature of the day underscores a dominant theme: the assumption that the profession would address—and if necessary remove—its outlier actors. Along with this was a bristly reaction to anyone outside the profession asking questions about problem physicians or questioning the efficacy of professional self-regulation.
To many retrospective observers, the Fifties ended in 1961 when America’s then-oldest president (Eisenhower) gave way to our youngest elected president (JFK). The quiet so often ascribed to the Fifties in popular culture was really more a matter of willfully overlooking some of the disquieting and disturbing issues that some preferred not to think about. The same might be said for medical regulation in the 1950s as a blithe professional attitude toward discipline soon gave way in the 1960s to a siren call: the medical profession and regulators had to clean up their act and make discipline a priority…or else.
The views expressed are those of the author and not the FSMB.
Sources:
See Chapter 6 of Johnson, Chaudhry. Medical Licensing and Discipline in America: A History of the Federation of State Medical Boards (Lexington Books, 2012)