We know a good deal about the early history and development of our system for medical licensure in this country. Historian of medicine Richard Shryock and medical regulator Robert Derbyshire1 contributed short but valuable works in the 1960s. Sociologist Paul Starr addressed licensing as one part of his masterwork on the social development on the medical profession.2 Scholars like Ronald Hamowy and Samuel Baker authored oft-cited journal articles looking specifically at the legislative origins and evolution of early medical licensure3 while the historian James Mohr explored the legal basis for medical regulation.4 What all of these authors contributed were broad brush stroke portraits of our medical licensure system—narratives delivering a valuable macro-level view of the subject.
What has been less frequently presented are state-level analyses of these origin stories for medical licensure. A scholarly few exist: Clinton Sandvick for Illinois, Samuel Baker for Massachusetts. Yet there is little in the scholarly literature that takes even a cursory look at the demographic profile of early licensees in any state. To put it bluntly, we have seldom posed the question, “Who were these guys?” (And yes, I know there were women too; small in number attempting to succeed in an entrenched patriarchal landscape)
The gift of a series of registry books from the Mississippi State Board of Medical Licensure to the FSMB Historical Collection provided me with an opportunity to explore that ‘Who were they?’ question directly. The donated volumes contained thousands of individual records assembled as part of a 1930s W.P.A. project for the Mississippi Department of Health—specifically individual applications for medical licensure in that state.
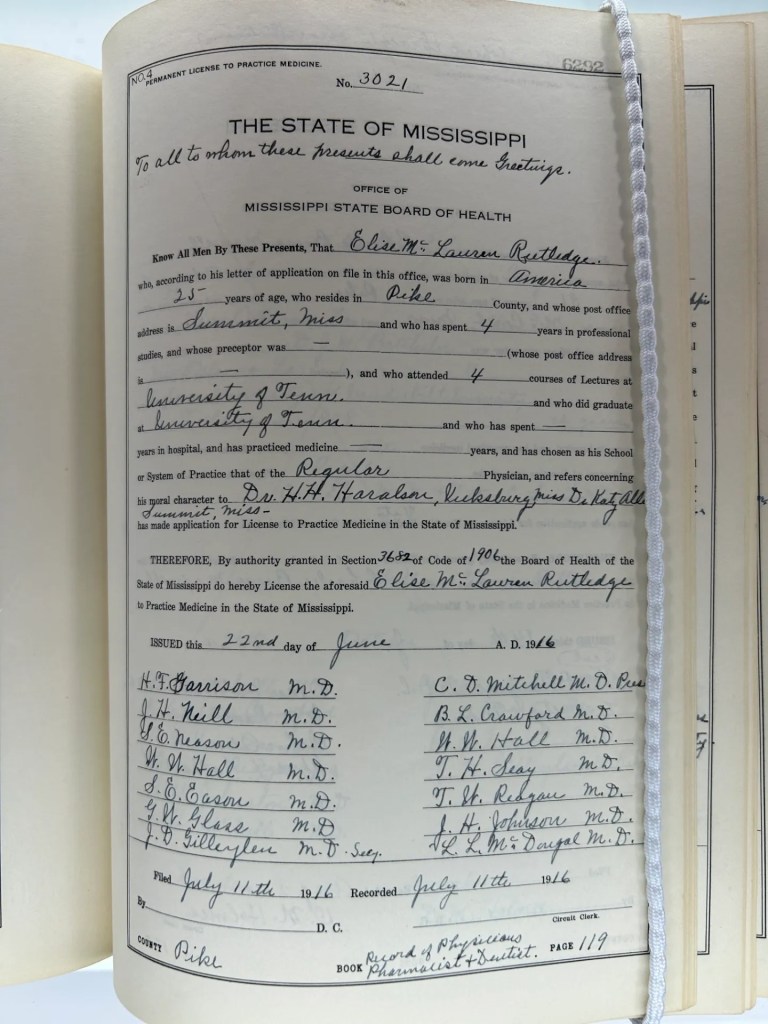
The time available to me precluded reviewing the entirety of the records contained in those volumes. Instead, I undertook a targeted, hopefully representative sampling from those volumes—approximately 472 records. What follows is a demographic summary of that sample set supplying insight into the early licensed practice of medicine in Mississippi. Who were they? Where were they educated? How much (in)formal training did they bring to their practice?
The 472 individuals were licensed over six decades (1882-1940). The majority of the records (80%) fell within the first three decades of that period. It comes as no surprise that the licensees over overwhelmingly male over this time span. Only six women were found to have been licensed in this sampling. Similarly, this sample found only four likely black physicians if we infer race from their associated medical school (Meharry-one of the historical black medical colleges).
While intra-professional strife characterized the relations between “regular” (i.e., allopathic) physicians and their “irregular” brethren for the second half of the nineteenth century, the small number of non-allopaths during this extended period (n=15) suggests these tensions may have minor irritants at best in Mississippi. The fifteen were categorized by the board as either eclectic, homeopathic, botanic or mineral physicians. Interestingly, no osteopathic physicians appeared in this data set spanning six decades.
| Time period | # of licensees | Holds Medical degree | Preceptorship | “Irregular” practitioners |
| 1882-1890 | 172 | 68 (39%) | 125 (73%) | 15 |
| 1891-1900 | 79 | 48 (61%) | 41 (52%) | 0 |
| 1901-1910 | 126 | 60 (47%) | 57 (45%) | 0 |
| 1911-1920 | 41 | 34 (83%) | 2 | 1 |
| 1921-1930 | 35 | 34 (97%) | 3 | 0 |
| 1931-1940 | 19 | 16 (84%) | 0 | 0 |
| Total 1882-1940 | N=472 | N=260 (55%) | N=228 (48%) | N=16 (3%) |
One question peaking my curiosity involved education—what type of medical education and training did these early licensed physicians bring to the treatment of their patients in Mississippi?
Only 55% of all the physicians in this sample reported having graduated with a medical degree. For those who did, where they attended medical school is worth sharing. Few of these physicians obtained their medical education and degree outside of the South. The medical colleges in Tulane and Memphis were the primary source institutions with 116 and 115 licensees respectively. Degree holders from schools in Louisville, Nashville and Jackson were smaller in number but still significant sources of the degreed-physicians in Mississippi.
Only 15 of these licensees presenting a medical degree obtained that credential from an institution outside of the South. Schools in Chicago, Cincinnati, New York City and Philadelphia predominated. (Note: My definition of the “South” included border states such as Missouri, Kentucky, Maryland)
If the strong southern orientation of the medical schools for these degree holding physicians didn’t surprise me, something else did: The number of individuals reporting medical education from more than one institution. More than one quarter (n=128) of the 472 physicians in the sample reported attending lectures at two or more medical colleges. While speculative, it may be surmised that repeating a set of didactic lectures at a second school was, if not common, then at least not unusual. Additionally, seeking clinical experience away from the school providing the core medical lectures seems understandable in an era when the onus for obtaining training fell more to the physician rather than their institution.
One of the more telling figures in suggesting the profoundly different educational landscape for medicine at that time involves the number of licensees presenting to the Mississippi board absent a medical degree. Less than half (46%) contained in this sample covering the period 1882-1910 possessed a medical degree.
This may seem strange to us today. However, like many states, the introduction of licensure laws in Mississippi included provision for licensing individuals who did not attend or graduate from a medical college.5 The reality is that such provisions were pragmatic in nature as state legislatures opted more often than not to grandfather in those individuals already practicing in the state who might not otherwise meet newly implemented requirements.
A total of 212 individuals reported no medical degree…and yet all but 27 of these physicians reported having attended at least one set of lectures at a medical college. Thus, licensed physicians who were wholly self-taught or trained solely via preceptor or apprentice relationships constituted only 6% of all the licensees in this sample.
The most common experience among the Mississippi licensees spanning these first three decades involved preceptorship. 59% of all the licensees during that period claimed one. Interestingly, familial connections may have played a prominent role in this as 55 of the 223 licensees did their preceptorship with a physician bearing the same last name. While some of these may have been coincidence, it seems likely that familial connection (father, brother, uncle, cousin) facilitated the training. The reported length of time under preceptorship seems not insignificant—a 3-years mean/median across the entirety of the sampling. Even if this self-reported data is inflated by half, it suggests that informal training occurred longer and more extensively than one might have thought.
One caveat to the preceptor data. This practice was common enough that it remained a standard field on the licensing application throughout the entire 1882-1940 time period. However, it was clear to me that some physicians (or the staff member filling in the form) classified the clinical portion of their medical education under the preceptor category. I excluded those instances where it seems clear this was being done.
So what to make of this data? Perhaps the key word to keep in mind is dynamic. This data, while specific to a single state, reflects the evolving nature of the medical educational and regulatory systems in late nineteenth and early twentieth century America—essentially a system in flux. Educational standards were still being formulated through a de facto accreditation process via the AMA Council on Medical Education and AAMC. Legislatures were following that lead by codifying these classifications for medical schools as the basis for licensure: Graduates of Class A and B schools as eligible; Class C graduates ineligible. Mississippi required graduation from a Class A school starting in 1919.6 Legislatures enacted and medical boards operationalized licensure requirements mindful of this still evolving educational landscape as well as the presence of thousands of established practitioners whose medical careers predated these changes.
Of course, we should be cautious in drawing conclusions from what is a sample set of data. Still, the data is consistent with what we would expect during a transition era in the history of the profession and the regulatory system. Perhaps an ambitious scholar would like to visit the FSMB Historical Collection and use these records for a more systematic survey and analysis?
The opinions expressed are those of the author and do not represent the views of the Federation of State Medical Boards.
- Richard Shyrock, Medical Licensing in America, 1650-1965 (Johns Hopkins, 1967); Robert Derbyshire, Medical Licensure and Discipline in the United States (Johns Hopkins, 1969)
- Paul Starr, The Social Transformation of American Medicine (Basic Books, 1982)
- Ronald Hamowy, “The Early Development of Medical Licensing Laws in the United States, 1875-1900,” Journal of Libertarian Studies, 1979; Samuel Baker, “Physician Licensure Laws in the United States, 1865-1915,” Journal of History of Medicine and Allied Sciences, 1984
- James Mohr, Licensed to Practice (Johns Hopkins, 2013)
- See Section 17 of An Act to Regulate the Practice of Medicine in the State of Mississippi (Jackson: State Printer, 1882)
- Mississippi Laws and Extracts of Laws Dealing with Public Health (Jackson: Mississippi State Board of Health, 1947), 104
