Behind every U.S. Supreme Court case there is a human story. It is easy to lose sight of that truth behind the Latin phraseology and abstract legal doctrines. Sometimes the humanity involved springs to our mind just from the name of the case: Brown v. Board of Education of Topeka Kansas (1954), Griswold v. Connecticut (1965) or Loving v. Virginia (1967). It is impossible to think of these cases without contemplating lives and stories of Linda Brown, Estelle Griswold, Mildred and Richard Loving.
Last time on this blog I discussed the little known but important U.S. Supreme Court case, Hawker v. New York (1898). With the legal elements of the case covered in my last post, this time we’ll explore the unexpected human story behind this case.
I started by looking again at the text of the Supreme Court case that infamized Dr. Hawker. To my surprise in re-reading the case, I realized that the court never identified Hawker by his full name or offered any biographical detail. They referred to him solely as “plaintiff” or “defendant” depending upon his status in the chain of cases leading to the highest court. Several cursory Google searches for Hawker v. New York proved unavailing as virtually everything I saw simply looped back to the same non-specifics in the text of the court decision.
I tried another tact. I used my Newspapers.com account to search for news stories on Hawker. I searched first for items appearing in 1898 to see if I could learn his full name. Easy enough –Benjamin Hawker (New York Times, March 10, 1898, p. 10) Then I searched New York papers for the1878 trial and conviction that figured centrally in the Supreme Court case. Cue flood gates opening! As I quickly learned, Dr. Benjamin Hawker appeared in newspaper stories as early as 1871 and often thereafter until his death in 1903. Hawker’s medical practice can be traced definitively to 1870 in New York (though I suspect it began even earlier) and continued for decades under several names: Dr. Benjamin Hawker, alias Dr. West, alias Dr. Perry.
(Note: To avoid confusing the reader, I will use the name Hawker throughout most of this post even when the cases involved his arrest as West or Perry)
Piecing together Hawker’s personal history required a good deal of patience in wading through scores of news items. Most of these dealt with a series of medical disasters resulting from his services to “Ladies in Trouble” (his October 18,1870 ad in New York Daily Herald). If we exclude the legal cases leading to the 1898 Supreme Court decision, a total of four cases constituted the bulk of this press coverage over the years The death of Emily A. Post (1871), the death of Christina Brecht (1876) and a pair of 1877 medical malpractice cases involving Maggie McLoon and Amelia Hyde. Further notoriety for Hawker stemmed from his 1894 arrest as part of a major police operation that swept up sixteen “malpractitioners”; and, of course, his 1896 arrest for violating state law that culminated in Hawker v. New York two years later.
As I parsed through all this material, I realized rather quickly that Benjamin Hawker was no medical innocent paying the price in 1896 for a single bad decision committed years earlier (1877). Nope. Hawker knew precisely the risks he took in the medical services he chose to provide. His eyes were wide open to the realities of medical jurisprudence in New York state…and he practiced accordingly as evidenced by his use of the Perry and West aliases.
So who was Benjamin Hawker? And where did he come from? How did he arrive at the practice of medicine in 1870? What kind of training did he receive?
Hawker was born in December 1837 at Somerset, England, one of six children to Hugh Hawker and Ann Sibley. His given name at birth was Benoni, a name of Hebrew origin. (Benjamin was the commonly adopted Westernized version of Benoni) Two of his older brothers shared names with similarly strong Biblical ties: Jabez, Theophilos.
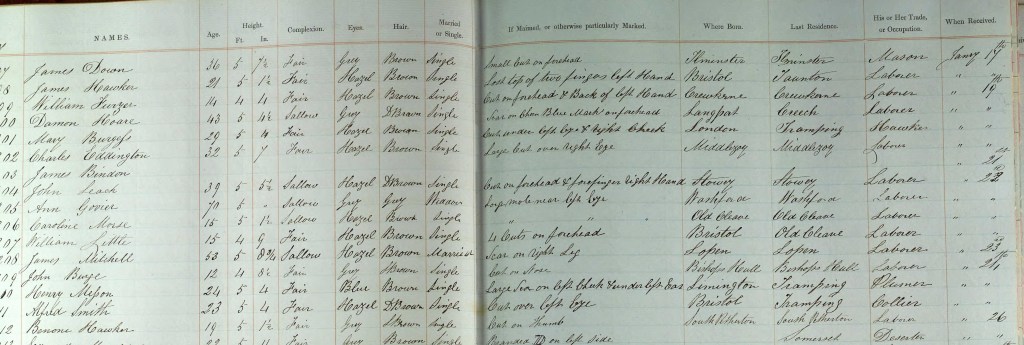
There is little else that can be said of Benjamin Hawker’s youth except that in 1857 he was committed to the Ilchester gaol in Somerset. His crime? Stealing two shillings from his employer which resulted in three months at “hard labor.”
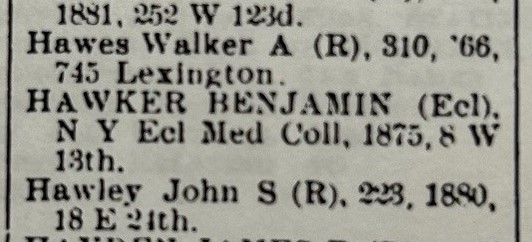
He arrived in the United States sometime in the 1860s. It is difficult to say when as a well-documented file in Ancestry.com identified an 1860 departure from England though Hawker later testified at an 1871 trial suggesting he arrived in the U.S. near the end of the Civil War. As part of that same testimony, Hawker claimed to hold a “certificate” from Guy’s Hospital (London) and to have been engaged in medicine for ten years. He acknowledged that he held no diploma though he asserted attendance at 2-3 medical courses. In 1876, he obtained a degree (or so he claimed) from New York Eclectic Medical College.
It is difficult to know how much of Hawker’s statements we can accept as fact. For instance, in that same 1871 testimony he acknowledged that his last name wasn’t Perry (the name under which he practiced medicine). In fact, he claimed his name was Benjamin Arthur. Was this further obfuscation on his part? Abandoning one alias for another? Perhaps except that “Benoni Arthur” can be found in the 1870 federal census for New York city. Occupation? stencil maker.
It seems unlikely to me that Hawker practiced medicine as a means of support in the years immediately following his arrival in this country. He may well have survived as a stencil-maker; then again, we know that in October 1870 he was operating as Dr. Perry from his office at 55 Bleecker Street. Equally plausible is the possibility that “stencil maker” was nothing more than a convenient lie to the census taker. And the name “Arthur”? Well…perhaps that was his middle name or perhaps he just made it up, like stencil maker.
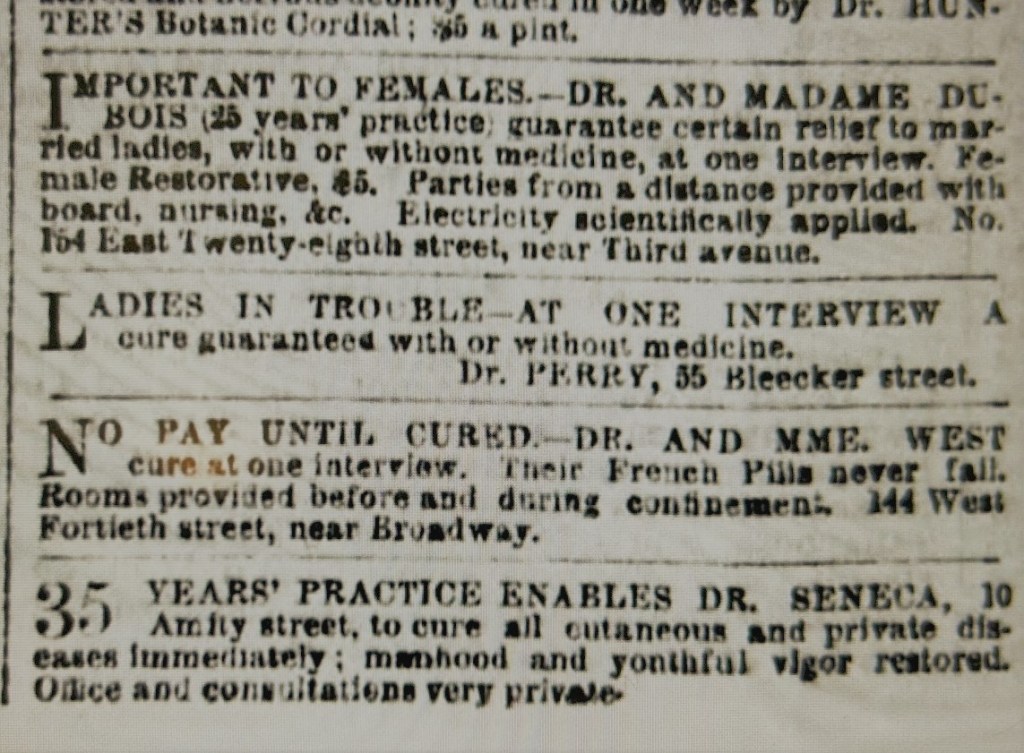
One thing is clear. Hawker kept offices on Bleecker Street throughout most of his career; and he often worked in conjunction with a female colleague. In the earliest years, this involved “Madame” Mary Van Buskirk; later this included Madame West, a woman named Mary Dunning or Gifford (accounts vary). His newspaper ads with the latter often stated that patients could “consult Dr. or Mme. West” at the Bleecker Street office.
Hawker’s first serious brush with the law as a physician occurred in 1871. Hawker and Van Buskirk’s efforts to terminate Emily Post’s late-stage pregnancy resulted in the death of both mother and child. The timing couldn’t have been worse for Hawker. His case overlapped with a lurid New York abortion death case, involving Dr. Jacob Rosenzweig (aka Dr. Asher) that captured national attention as the trunk murder mystery. In September 1871, a jury convicted Hawker of 4th degree manslaughter and applied the maximum sentence: two years imprisonment. In a separate trial, his colleague Madame Van Buskirk walked after a hung jury.

By 1874, Hawker was out of jail and back in practice at his Bleecker Street address, Now, however, he practiced as Dr. West based upon his advertisements in the local papers. The death of one his patients, Christina Brecht, in February 1876 and her deathbed confession brought local authorities to Hawker’s office doorstep once again. Two elements are worth noting from this case.

First, if Hawker had hoped to cover his track through the use of a new alias (Dr. West), events soon proved him wrong. His alias cover fell apart quickly as within a few days, the arresting officer from Hawker’s 1871 case identified him as “Dr. Perry” from Emily Post’s death.
The second unusual element was the quiet dismissal of the Post case despite significant press coverage in February-March 1876. After May, the case disappeared from the press. I could find no subsequent references to the case that ever mentioned a trial or conviction. I can’t help wondering if Hawker’s allegedly healthy holdings in three different banks may have assisted him in discreet, behind the scenes fashion. The Philadelphia diploma mill criminal John Buchanan effectively deployed such a tactic to help legal paperwork disappear after greasing the palm of city clerks or aldermen. I suspect such possibilities existed in New York as well. The later 1895 NY Senate hearings under the Lexow Committee scandalized New York with its documentation of corruption (bribes, kickbacks) to police and others as a means of forestall scrutiny and arrests against physicians like Hawker providing illegal services. (Hawker appeared before the committee; his rival Newton Whitehead (see below) became a major witness)
As the various medical ads in the New York newspapers indicate, Benjamin Hawker had plenty of competition in drawing patients for his services. In 1877, Hawker fell into a protracted bitter rivalry with another physician, Dr. Newton Whitehead—an almost irrational rivalry whose end result saw Hawker convicted and sentenced in 1878 to a long prison term.

The bizarre series of reprisals between the two started in September 1877 when a disgruntled former patient of Hawker’s (Maggie McLoon) made her way to the office of Dr. Whitehead. She complained that Hawker relieved her of $50 (“all she had”) yet failed through his “operation” to terminate the pregnancy. Whatever the source of the enmity between the two men, Whitehead saw this as an opportunity to strike against Hawker. He escorted McLoon to an attorney promising she would “get justice.” The subsequent arrest of Hawker, Madame West and another associate led to the two doctors filing a series of legal complaints and counter-complaints with the courts. The headline of an October 3, 1877 news item summarized it best, “Doctors Quarreling.”
Matters only accelerated when Whitehead induced another Hawker patient, Amelia Hyde, to press charges related to an operation he performed on her. When Hyde failed to appear for the hearing, the case seemed dead–or so one would think. However, not yet content and eager to inflict his own blows against Whitehead, Hawker responded by filing a conspiracy charge of his own against Whitehead and Hyde. On the day of the hearing, Hawker went to court ready to support his conspiracy charge only to find that Ms. Hyde had shown up this time…and she was anxious to testify to Hawker’s medical malpractice.
The DA and judge resurrected the earlier dismissed case when Hyde failed to appear. This time Hawker’s luck ran out. Even the services of former New York mayor Oakley Hall, serving as Hawker’s attorney, couldn’t save him from a jury and press eager to see Hawker in the docket. Hawker played his last card—pressing charges with a resulting arrest of Dr. Whitehead—intended to keep his rival from testifying along with Hyde at his trial. All of this proved to no avail as the jury convicted him on March 1, 1878.
An unsympathetic judge sentenced Hawker, stating…:“Hawker, you have been convicted after a fair and impartial trial, upon an indictment for producing an abortion upon Amelia Hyde. You have been defended by one of the most famous lawyers in the country, but the jury convicted you. Upon that charge you are sentenced to be imprisoned in the King’s County Penitentiary for the term of ten years. That is all.”
Newspapers and social critics lauded the conviction. The Brooklyn Times Union congratulated District Attorney Isaac Catlin for producing the conviction, using almost precisely the same available evidence, that his predecessor Winchester Brinton had failed to secure. Anthony Comstock, leader of the New York Society for the Suppression of Vice, echoed the chorus lauding Catlin for securing a conviction.
In a letter published soon thereafter, Comstock told Catlin…“You started the ball in motion against this class of criminals, which, I trust, will not stop until every scoundrel in this damnable business of child murder gets his deserts. The public owe you and his Honor Judge Moore more than congratulations or thanks in this case.”

Hawker and his attorneys filed various appeals—all of which failed. Hawker appears to have served the entirety of the ten-year sentence.
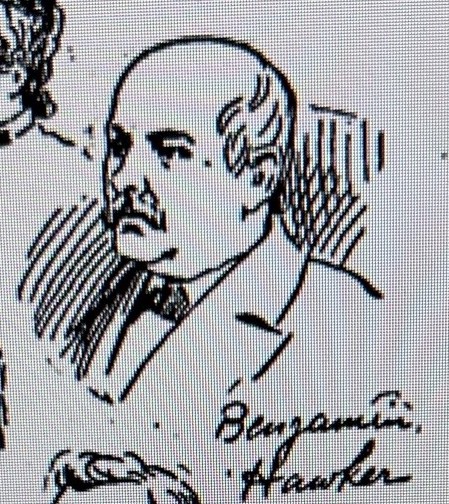
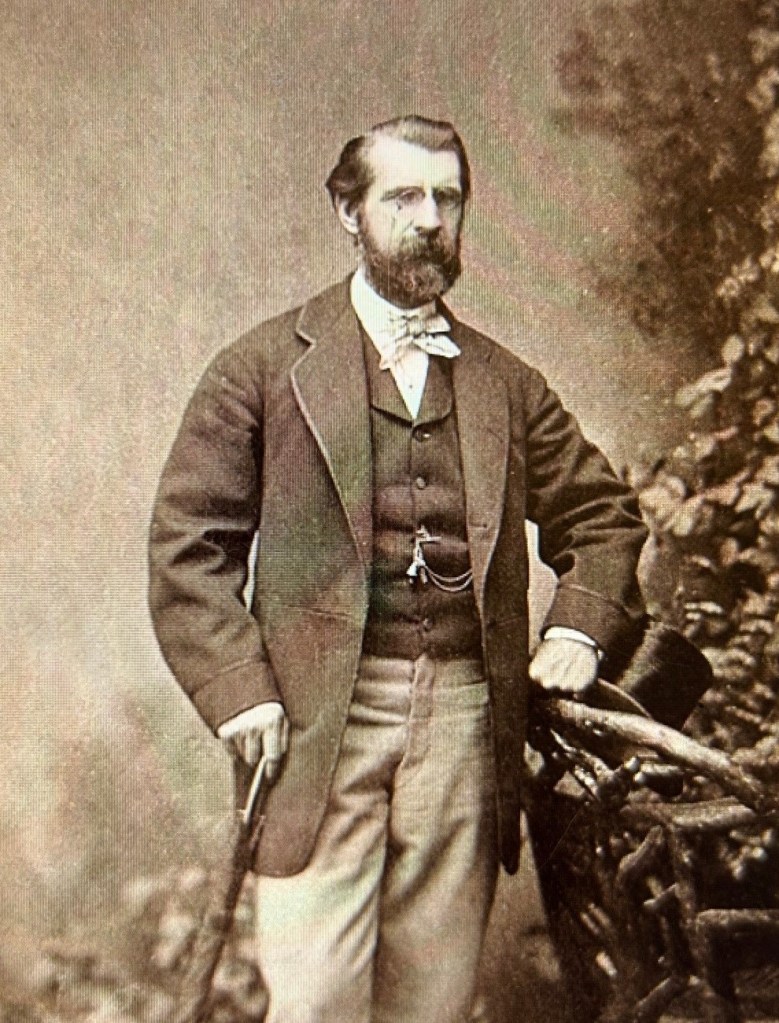
A decade spent in prison appears to have changed Hawker little—or perhaps he couldn’t envision any way to reinvent himself or make a living other than what he had by doing since 1870. In 1894, he and Whitehead were among the sixteen physicians, midwives and other self-styled doctors caught up in a police raid targeting medical “malpractitioners.” The assistance of an agent from the Society for the Enforcement of Criminal Law ensured major press coverage that included the New York World’s sketch artist presence at the chaotic court room scene. He quickly sketched the more infamous suspects, including Benjamin Hawker. This hastily drawn image is the only likeness of Hawker known to exist. Hawker posted $2,500 bail and disappeared.

Arrested two years later in 1896 for violating the state law barring felons from medical practice (described in my prior blog post), the legal path began that would take Hawker’s case all the way to the Supreme Court.
Hawker seems to have settled into a discreet medical practice in the aftermath of these legal decisions and effectively stayed off the radar of the authorities. He apparently supplemented his income by housing boarders at his home. His legal tribulations still weighed heavy with him as evidenced by his pursuit, and acquisition, of a commutation from New York whereby the state “restored [him]to all rights of a citizen.”
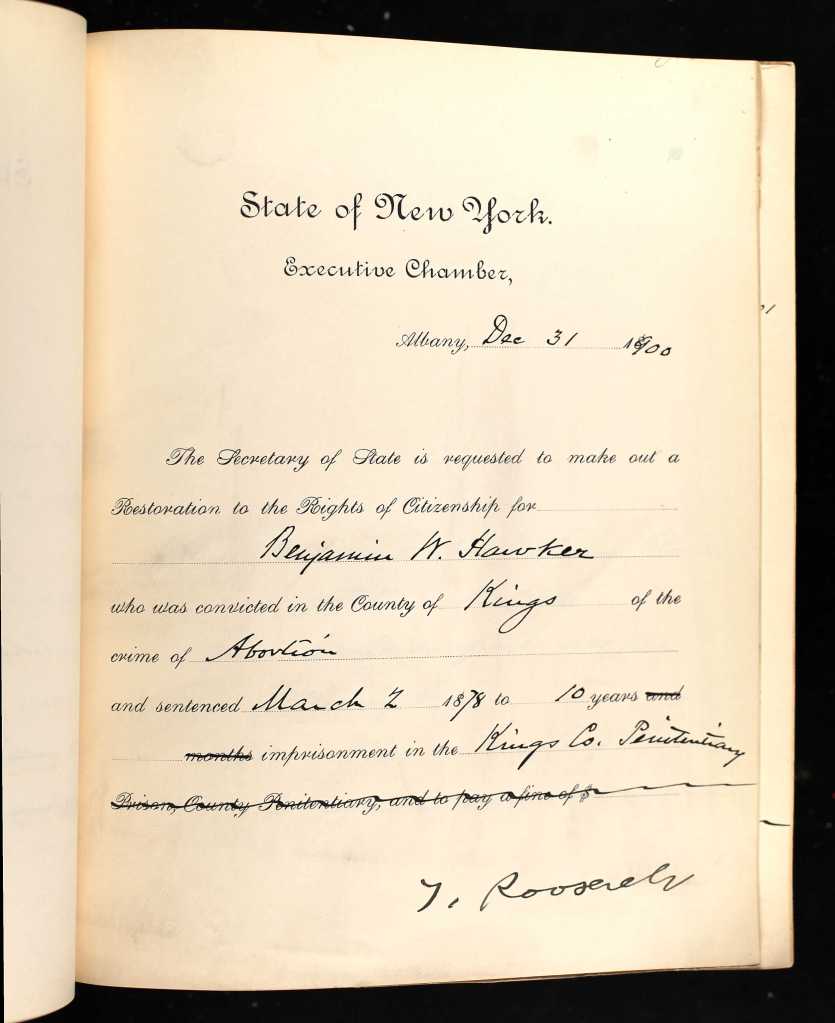
Gov. Teddy Roosevelt’s signature
In June 1903, Hawker reappeared in the news in shocking fashion–as the victim of a brutal assault that occurred from a botched home-invasion robbery.

A former boarder, Dudley Bartlett, and his accomplice made plans to surprise, force him to open his safe and then chloroform him before making their escape. Little went according to plan as the accomplice bolted when Hawker and Bartlett engaged in a violent struggle for the gun. Repeated blows to the head and neck left Hawker badly injured and Bartlett apprehended.
Benjamin Hawker died at his home about six weeks later. The coroner attributed death to a diabetic coma, insisting—after consultation with Hawker’s treating physician, that the death was unrelated to the assault and injuries sustained six weeks earlier.

I’m torn as to what to make of Dr. Benjamin Hawker and his career. My curiosity about him stemmed simply from wanting to know the human story of the man behind a key Supreme Court case in the field of medical regulation. I wasn’t sure what I’d find in looking for him. I didn’t expect to find…well, I’ll just call him what many would—a career abortionist. Though I find myself loathe to condemn him with the sweeping moral assertions that some would impose.
Then again, perhaps nothing I found should surprise me. The lives of real people and their life trajectory rarely fit into tidy retrospective categories and labels. Life is messy; history is equally so.
The opinions expressed are those of the author and do not represent the views of the Federation of State Medical Boards.
Sources:
“The Brooklyn Abomination,” New York Daily Herald, August 31, 1871, p.6
“Medical Murder,” New York Tribune, September 2, 1871, p. 2
“The Courts,” Times Union (Brooklyn), September 23, 1871, p. 3
“The Courts,” New York Tribune, September 25, 1871, p, 2
“Medical,” New York Daily Herald, February 8, 1874, p. 16
“Dr. West,” Brooklyn Daily Eagle, March 3, 1876, p. 4
“Brecht Malpractice Case,” New York Times, March 5, 1876, p. 12
“Charged with Malpractice,” New York Times, September 20, 1877, p. 8
“Doctors Quarreling,” New York Times, October 3, 1877, p. 2
“Doctor Perry,” Times Union (Brooklyn), January 29, 1878, p. 4
“Another Chance for ‘Vindication’,” Times Union (Brooklyn), March 4, 1878
“The Courts,” Times Union (Brooklyn), March 6, 1878, p. 4
“Brooklyn,” New York Times, March 10, 1878, p. 2
“Charged with Malpractice,” Brooklyn Daily Eagle, March 24, 1894, p.12
“Held for Awful Crimes,” New York World, March 25, 1894, p. 13
“Physician Assaulted and Brutally Beaten,” New York Times, June 28, 1903, p. 2
“Physician was Careful,” New York Sun, August 3, 1903, p. 10