It is human nature to crave certainty…to seek a clear understanding of our world and definitive answers to the questions—big and small—that confront us. There’s a reason for this. Science suggests strongly that we, as humans, are fundamentally hard-wired to seek answers or explanations. Indeed, even when these are not available or immediately apparent, our minds work actively to supply them. Along the way is an accompanying human tendency toward reductivist thinking—the tendency to take complex questions and issues and rework them in order to reduce them to ones offering simplified, general answers.
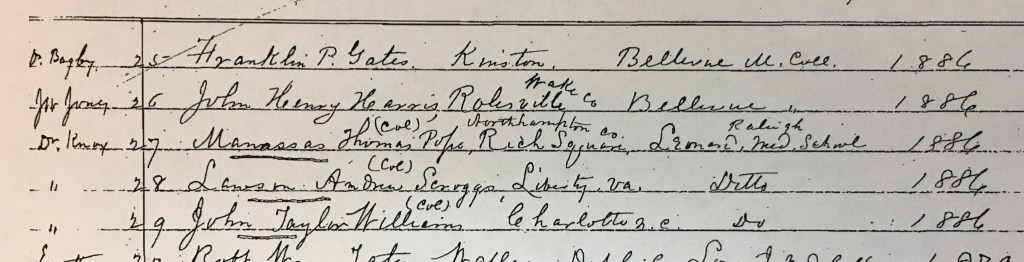
I offer this as preface to my update from an October 2018 blog entry titled, “Bias in Testing?” In that post from three years ago, I discussed a research project I had undertaken—one looking at the Register (official record) from the North Carolina Medical Board triggered by my finding that for nearly fifty years the board’s practice had been to annotate the record of black physician candidates for licensure. The board annotated these physicians’ record with “c,” “col” or “colored.”
I wondered whether this was a striking but ultimately benign action consistent with administrative practices in other state agencies in North Carolina? Or did this flagging point toward bias in the examining and licensing of these physicians? My research is complete and now appears in the current issue of the North Carolina Historical Review.
Like so much of history, “facts” do not necessarily speak for themself. I know some may balk at this statement fearing it justifies revisionist historical narrative. I will be blunt in my response. That kind of knee jerk reaction championing “facts” reflects a fundamental misunderstanding of the nature of historical inquiry. Placing evidence within an appropriate historical context requires the active participation of a human being —specifically the overlaying element of interpretation of the facts, findings, documents, evidence, etc. Quite simply, someone has to place research findings within a narrative framework to communicate to the rest of the world, whether fellow scholars or the public.

As the historian Nancy Partner once wrote, “Archives contain many interesting things but Truth is not included among them.”
So what did I find in looking at scores and performance on North Carolina’s licensing exam over forty years (1886-1925)? Let’s start with this.
Data analyses showed the exam performance by graduates of historical black medical colleges (HBMCs) as consistently lower than that of graduates from non-HBMC schools throughout the period studied. Those who would argue for letting the “facts” speak would likely point to this data as direct evidence of bias in the North Carolina exam. You may even agree.
But before you leap to that conclusion, what if I told you that the scoring for these exams (comprised of extended response or essay questions) was done in a blinded fashion? The candidates for licensure by examination were issued either a pseudonym or a number by the board Secretary on the day prior to testing. The examinees used this identifier, rather than their actual name, on their examination papers. Thus, the board member scoring the test ostensibly did not know the identity of the examinee.
You may be thinking several things now. After all, we have the advantage of historical hindsight. We know the segregated nature of much of America at that time so you might ask, “How can we be sure the board followed this safeguard consistently?” Or you might ask, “Wasn’t the board Secretary still in a position where he knew the identity of the examinees?”
Those are fair questions. All we know is what was preserved in the board’s records documenting this process. Absent evidence to the contrary—letting the facts speak without the historian’s involvement as some would demand—means we start with a presumption that this safeguard was followed. Hopefully, however, some of you are thinking again about that Truth and the archives quote.
Let’s consider another question. If we accept the scoring safeguard used by the board and thus the legitimacy of the data, how do we explain the discrepancy in HBMC performance? In the article, I treat this question at length and find strong evidence from contemporary black educators suggesting the performance differential stems from significant challenges presented to HBMC matriculants by inadequate pre-medical education and financial/resource constraints facing these schools. The records of administrative officials at HBMCs are rife with concerns these realities presented in preparing their graduates for state board licensing exams.
Now let’s turn to a second finding from this research. Graduates of HBMCs showed a higher pass rate on the North Carolina exam relative to their performance on other states’ licensing examinations. Indeed, the performance of HBMC grads on the North Carolina exam exceeded (by 12%) the overall pass rate on state board exams collectively during this time period. In essence, the North Carolina presented “no greater hurdle” to licensure than that of most of states.
If we let the facts speak for themselves, this finding suggests that conscious, overt bias in scoring the exam—if it existed—did not play as extreme a role as we might have thought. But as an historian of medical regulation, I am uncomfortable in stopping there (i.e., simply accepting the facts) as opposed to contextualizing this finding.
Black physicians of this era viewed state licensing exams cautiously and with an understandable degree of skepticism. Who wouldn’t wonder what kind of standard was being applied when the New Orleans Medical and Surgical Journal reported that 70% of the 257 applicants for licensure failed Mississippi’s exam in summer 1907 and then nearly 80% passed in December?

The insular nature of the medical boards (almost exclusively all-male and all-white) meant that those outside those demographics held understandable reservations about fairness. What was the purpose of an annotation to a record if not to clearly make someone, in a position of authority and/or control, aware of the race of the licensure applicant? Here I can’t help but remember the story shared by the first black woman licensed in Colorado in 1902. That board’s executive secretary expressed reluctance to accept her license application and fee. With total candor he said, “You’ve got two strikes against you. First off, you’re a lady and second, you’re colored.”
The annotation practice itself? It appears to have been…well, if not ubiquitous, then certainly common enough that it triggered no contemporary comment. The North Carolina nursing board during this period annotated their records for black nurses as well. Updates on state board exams published in medical journals include numerous instances in which “colored” examinees’ performance is called out explicitly.
Thus, even though I had a significant amount of data (“facts”) at my disposal, I found it challenging to present my findings—sometimes mentally second guessing myself in my interpretations. For example, the board’s Register documented a single segregated administration of their exam in 1886, the first year an HBMC grad presented for licensure. The Register doesn’t record a segregated administration again. Does this mean this practice stopped after 1886? Or was it a continued practice so administratively unimportant (or socially presumed) that it didn’t merit documenting in the Register?

And what about the role of the board Secretary? The board’s blinded scoring protocol operated as intended only to the extent that the person serving in that role behaved in a manner that preserved the de-identification until after scoring had been completed. Said another way, the efficiency of this safeguard rested upon the integrity of one man. Where does that leave the historian? Am I naïve in presuming the integrity of this safeguard? Is it fair for me to cast suspicion based upon performance differential alone if no other evidence exists suggesting the safeguard was not being utilized?
I found this research project to be both fascinating and discomforting. In 2021, questions of race—even when seen through the lens of an exam discontinued long ago—cause many to give pause and tread lightly. I had professional colleagues reluctant to collaborate on this research project. I had one medical board executive director express early interest in a similar project with their board’s exam; then disengage entirely after I shared details of the North Carolina project. I understand the reaction in both instances.
I hear Nancy Partner yet again: “Archives contain many interesting things but Truth is not included among them.”
In the final draft of the article sharing my findings, I found myself acknowledging an uncomfortable truth common to historical research and writing. “…neither this study’s data analyses nor documentation from the time period provide unambiguous evidence.”
The opinions expressed are those of the author and do not represent the views of the Federation of State Medical Boards.
Sources:
David Alan Johnson, “The North Carolina Medical Licensing Examination, 1886–1925: Analysis of Performance by Examinees from Historically Black Medical Colleges,” North Carolina Historical Review, April 2021 (152-182)
