“An institution is the lengthened shadow of one man.” Ralph Waldo Emerson, Self-Reliance, 1841
I remember coming across this quote many years ago and being struck by its pithy expression of a profound truth. One that many of us do not fully appreciate until later in life—when our own experiences and accumulated years bring an understanding that the vagaries of human existence make it all the more remarkable when any company, organization or institution manages to survive beyond a few decades. Longevity stands out in a world littered with Kodaks, Sears planned obsolescence and unanticipated technical disruption.
Approaching retirement from the Federation of State Medical Boards (FSMB), I cannot help but reflect on the trajectory of my career and the organization that did so much to foster it. Nearly 29 years with the FSMB has offered a life lesson in the ebbs and flows that are a natural part of the life cycle of any long-standing organization. I’ve seen leadership navigate challenges large and small over nearly three decades. Success—both immediate and long-term—is seldom accidental, but the result of a clear vision, steady temperament and a dash of good luck along the way.
I share this because my knowledge of the history of FSMB and medical regulation in this country underscores that some institutions emerge from specific circumstances and survive—as Emerson suggests—due largely to the contributions of a single individual. This blog post represents the first in a series spotlighting the impact of several individuals who proved instrumental to the history and development of medical regulation in this country.
Walter Bierring, MD (1868-1961)
Let me start by saying that I and all my FSMB colleagues should thank Walter Bierring for our jobs. It is not an overstatement to say that if not for him, the FSMB probably would not exist today.
An intellectually curious and ambitious son of Danish immigrants, Bierring attended medical school at the University of Iowa and later pursued training in Europe: Heidelberg (1892), Vienna (1896), Paris (1901). Bierring worked as a medical educator (Univ. of Iowa; Drake) until 1913 when his focus shifted toward professional and regulatory interests. His addition to Iowa Board of Health and later the state medical board brought him directly into the orbit of the FSMB.
Bierring’s talents and leadership were quickly recognized. In 1916, FSMB President Charles Cook wrote Bierring to confide his belief that the latter was key to the organization’s ultimate success.
“The future of the Federation, as I see it, is today largely in your hands…you know its past history, the pitfalls to be avoided, the problems to be solved, lines of work to be taken up, the danger of its being over-shadowed by other organizations….”
Cook’s prophecy held true. Bierring served as the FSMB Secretary-Treasurer from 1915-1960 and as the editor of the Federation Bulletin during nearly all of that span of time.
Why was Bierring so integral to the FSMB’s success and survival? It’s simple. He served as the key player sustaining the organization at a time when it had no full-time paid staff, no permanent national offices, no specific product/service generating revenue and minimal resources derived from modest membership dues and in-kind resource assistance from the AMA. For more than 45 years the “work” of FSMB was largely sustained by this one man from his home in Iowa. Bierring carried the FSMB through its most trying times in the 1930s and early 40’s. For all intents and purposes, Bierring was the Federation during the organization’s leanest years.
Looking back, it is easy to see that the organization might have slipped into a moribund condition and total irrelevance. Indeed, it might well have collapsed entirely without him. Knowing the FSMB today, this seems unimaginable and yet such an outcome was clearly possible, and ultimately avoided, due largely to Bierring’s contributions and steady hand over four decades.
So how did he do it? Patience, dogged persistence and force of personality. Bierring’s leadership style mirrored the attributes identified by business writers as critical to successful CEOs: humility, curiosity, a collaborative-spirit. Despite the accolades that came his way, Bierring shared credit freely with his colleagues. Over the years he wrote a series of articles highlighting the contributions of other FSMB colleagues. Bierring preferred winning over opponents through reasoned conversation and a bit of charm. As one of his contemporaries described him, Bierring was “always constructive, never destructive.” He preferred quiet diplomacy to direct confrontation—what today we call consensus-building.
When necessity arose, he could be forceful in his own way—particularly in exerting influence. One contemporary described his approach as an “iron fist in a velvet glove.”
Bierring didn’t innovate a product or service; he didn’t blaze new trails on the policy or legislative front. What he understood best was people and how to work with and through them for a desired goal—and at the right pace. For the leader of any membership organization this is a critical skillset. Operating in such a way that you are neither too far in front nor so far behind that you risk losing those you are seeking to lead.
Walter Bierring represented the longest single strand of continuity linking the organizations from its earliest days to the cusp of its resurgence in the early 1960s into the modern organization that exists today. If not for Walter Bierring, it’s unlikely the FSMB would have survived long enough to enjoy that reemergence.
Perhaps a former FSMB President said it best: “…the most fitting and lasting tributes to Dr. Bierring is the Federation itself. This is his true testimonial…he has laid the foundation and it is up to us to build and carry on.
Thank you, Dr. Bierring.
The opinions expressed are those of the author and do not represent the views of the Federation of State Medical Boards.
Source:
This blog post is adapted from chapter 5 of Medical Licensing and Discipline in America: A History of the Federation of State Medical Boards (2012)
My last several posts drew inspiration from materials donated by the Mississippi Board of Medical Licensure to the FSMB Historical Collection. I used a representative sample set drawn from license applications submitted to that board as a means of exploring the demographics of the early physician licensees in Mississippi. My last blog post addressed test construction and performance data on the Mississippi exam spanning the period from 1924-1958.
Today’s post focuses on the actual questions presented on the Mississippi exam. As my colleague Cyndi Streun, D. Eng., and I perused the two-volumes containing all the Mississippi board’s test questions spanning 1924-1958 any number of questions came to mind. We wondered if these were quality test items? Did they require candidates to apply relevant medical knowledge? Or were they exercises in recall asking for factoids and medical trivia? In essence, we wondered “How good was the exam?”
To answer these questions, we sought formal review from a group of subject matter experts (SMEs): licensed physicians. The four physicians who participated with us all held ABMS certification in either family medicine or internal medicine; and they all had experience in assessment through their service as committee members working on the United States Medical Licensing Examination® (USMLE®).
The sheer volume of questions available for review presented both an opportunity and a quandary. There were more than 3,900 test questions available to us with three hundred or more items in each of the subject areas, e.g., anatomy, physiology, surgery, etc. Even reviewing all the test items from a single year meant asking an SME to read and critique roughly 80 or more questions. In order to make this task more manageable for these SMEs volunteering their time, we settled upon a small subset of questions from a single subject area.
The SMEs reviewed 56 physical diagnosis questions drawn from multiple administrations of the Mississippi board’s medical licensing exam spanning over thirty years. We pulled items from this subject area of the test administrations from 1925, 1930, 1935, 1940, 1945, 1950 and 1955. Each SME reviewed these questions independently. For every test item they applied a Yes/No response to a series of prompts.
Is the question clinically relevant?
Is the question appropriate for inclusion on a medical licensure examination?
Does the question involve clinical reasoning?
If the SME answered affirmatively for clinical reasoning, they were then asked to assign a specific level from Bloom’s taxonomy (i.e., remembering, understanding, analyzing, applying, evaluating, creating) to their rating of the question.
This methodology allowed us to provide a consensus score for the SMEs’ collective rating of each test item. Perfect agreement with all raters answering yes would be a 1.0 score for that test item. Three of four raters saying yes equaled 0.75, etc. The same approach was used to attach a score to appropriateness for a licensing exam and whether clinical reasoning was required. As an example, perfect agreement among the raters for clinical relevance would be a score of 8 in 1925.
There was no perfect consensus among the four raters for any of the three categories in any of the years in this study. In general, the SMEs’ retrospective review deemed the Physical Diagnosis questions clinically relevant (overall .85) and appropriate for a medical licensing exam (overall .78). See Table 1.
Table 1: SME evaluation of clinical relevance, appropriateness and clinical reasoning on 56-test item set drawn from Mississippi’s medical licensing exam
# items
Relevance points
Appropriateness points
Clinical reasoning points
1925
8
5.75
5.5
3
1930
7
6.25
6
4.75
1935
8
7
6.75
4.25
1940
8
7
5.75
4
1945
9
8.5
7.75
5
1950
8
7.5
6.25
5.25
1955
8
6
6
3.5
total
56 questions
48 pts
44 pts
29.75 pts
0.857 avg
0.785 avg
0.531avg
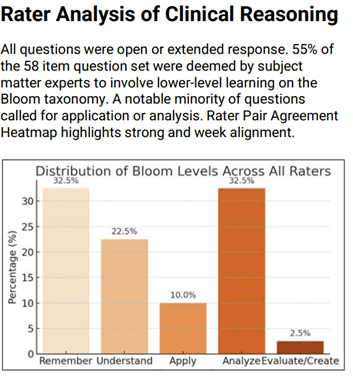
The SMEs judged clinical reasoning as the weakest of the three domains considered. Indeed, this area proved challenging for the SMEs themselves as it is clear that some did not view the lowest levels on Bloom’s taxonomy (remember, understand) as falling within their own definition of clinical reasoning in a medical context.
We quantified the application of Bloom’s taxonomy by identifying instances in which two SMEs marked the same question as requiring a higher clinical reasoning (analyze, apply, evaluate). Only 12 of the 56 test items met this threshold.
To the extent clinical reasoning was deemed by the SMEs as being required of the examinee to answer the question, it was generally seen as occurring at the lower levels on Bloom’s taxonomy (remember, understand). The SMEs assigned the lowest levels (remember, understand) on Bloom to 55% of the total 56 test items.
So what might we surmise from all of this? Several things but first let’s be clear on the limitations of what I’ve shared. This project involved a subset of test items from a single subject area (Physical Diagnosis). More ambitious work might tackle all 300+ test items from a single subject area…or all the questions posed from a single year’s test administration…or from multiple administrations of the Mississippi exam. And while there is nothing to suggest that Mississippi was unique in the construction and content of its licensing examination, this remains a snapshot from a single state.
Having said all this, several things are worth stressing. It seems fair to say that our SMEs had generally positive views for the appropriateness of the questions being asked and their clinical relevance. In essence, what was being asked seemed reasonable even though the questions did not consistently and routinely require candidates to apply their knowledge.
It is also fair to say that these test items (and the examinations in general) were very much products of their time. On multiple occasions the SMEs called out “antiquated” or “dated” language or that today one would apply a “more specific diagnosis.”. The SMEs flagged instances in which a question might be far less relevant today than at the time it was used on this exam. For example, a question diagnosing typhus or rheumatic fever today (compared to the 1930s) might feel like “esoterica.” Additionally, imaging and lab tests would be the standard approach today for conditions previously diagnosed through physical findings several generation ago.
Indeed, one of the major challenges that arose early in working with the SMEs was agreeing upon the lens through which their evaluation should be made—specifically, was the SME rating these questions for appropriateness, clinical relevance, etc. through the lens of medicine as taught and practiced today? Or through the lens of what was understood and practiced at the time of the test? Ultimately, we directed the SMEs to evaluate the test questions through the lens of medicine today. The rationale being that we did not expect our SMEs to be historians of medicine evaluating each item through the lens of medical knowledge known at specific points in time spanning mid-20th century America.
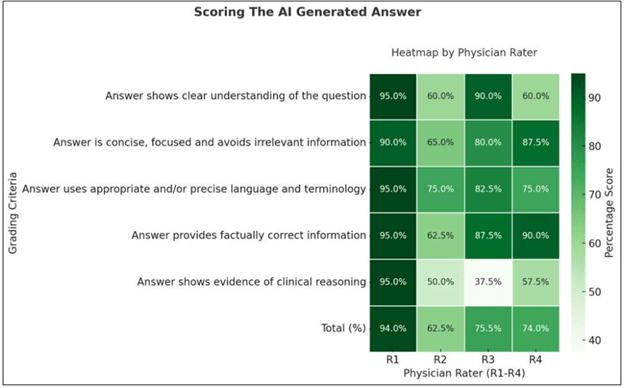
A final element of this study involved using an AI-model to generate answers to each of the 56 physical diagnoses questions drawn from the Mississippi exam. We then asked our four SMEs to rate the AI-generated answers. Our SMEs evaluated the AI-developed answers based upon the following criteria:
Did the answer show a clear understanding of the question?
Was the answer clear, concise and without irrelevant information?
Did the answer use appropriate language and terminology?
Did the answer provide factually correct information?
Did the answer show evidence of clinical reasoning?
Our SME human raters scored AI generated answers to the dataset questions highest in providing factually correct information, using appropriate language and avoiding irrelevant information. Our SMEs showed markedly different views of the AI answers in their demonstrating clear understanding of the question. Finally, and perhaps not surprisingly, our SMEs scored the AI-generated answers lowest for showing evidence of clinical reasoning. (see below)
Final reflections:
Mississippi’s approach to assessment was conventional and consistent with long-standing state board methods (extended response test items). It was also vulnerable to the deficiencies inherent to that format, e.g., reliability. The board members were not measurement scientists and perhaps not even expert in the subject area(s) they were asked to write test items.
The questions posed on the Mississippi exam were generally relevant and appropriate to a licensing examination. They may not have required the physician candidates to consistently apply a high degree of clinical reasoning but, based upon my familiarity with medical licensing exam questions in other states, the Mississippi exam seems no better or no worse in that regard than other states.
Perhaps most important was the standard being applied as evidenced by the pass rate on the Mississippi exam. It seems clear that regardless of what was being asked on the exam, the depth and breadth of knowledge deemed acceptable as evidence of proficiency was an easily achievable hurdle for nearly all the Mississippi candidates in most years. Remember, Mississippi passed every candidate tested on their exam in 23 of the 35 years in this study. Only 1.3% of all their candidates were failed by the Mississippi board.
Finally, we’ve all heard an iteration of the quote describing medicine as a blend of science and art. If so, it seems that testing during the era of state medical licensing exams probably belonged as much to the latter as it did to the former.
The opinions expressed are those of the author and do not represent the views of the Federation of State Medical Boards.
I’ve written before about the donated materials contributed by the Mississippi Board of Medical Licensure to the FSMB Historical Collection (FHC). https://armchairhistorian.blog/2025/10/07/preserving-the-history-of-medical-regulation/ Among the donated materials are a two-volume set containing all the questions (organized by year and subject area) presented to candidates on that state’s medical licensing exam between 1924-1958.
This gift piqued my interest as well as that of a colleague. As we considered the source materials donated to the FHC, various ideas and questions came to mind: How challenging were these state-developed medical licensing exams? Were they quality exams requiring candidates to apply relevant medical knowledge? Or were they exercises in recall too often seeking factoids or obscure medical trivia? There was a lot riding on the outcome of these exams—a medical license, a career and professional livelihood. So were these exams constructed, administered and scored in a manner commensurate with the high-stakes nature involved with the licensed practice of medicine?
We undertook something akin to a case study of the Mississippi licensing exam, blending two approaches: (1) AI and human rater analysis of these the Mississippi test questions, and (2) review of performance data on the Mississippi exam. My next blog post will share some of what we learned about the former. Today, I want to focus on this latter, starting with how these exams were constructed.
Structure and format of the Mississippi exam
From its originating legislation in 1882, Mississippi required physicians to pass a written examination conducted by its examining body. (Note: There was an exemption in this original law that allowed established practitioners in the state to forego the exam).
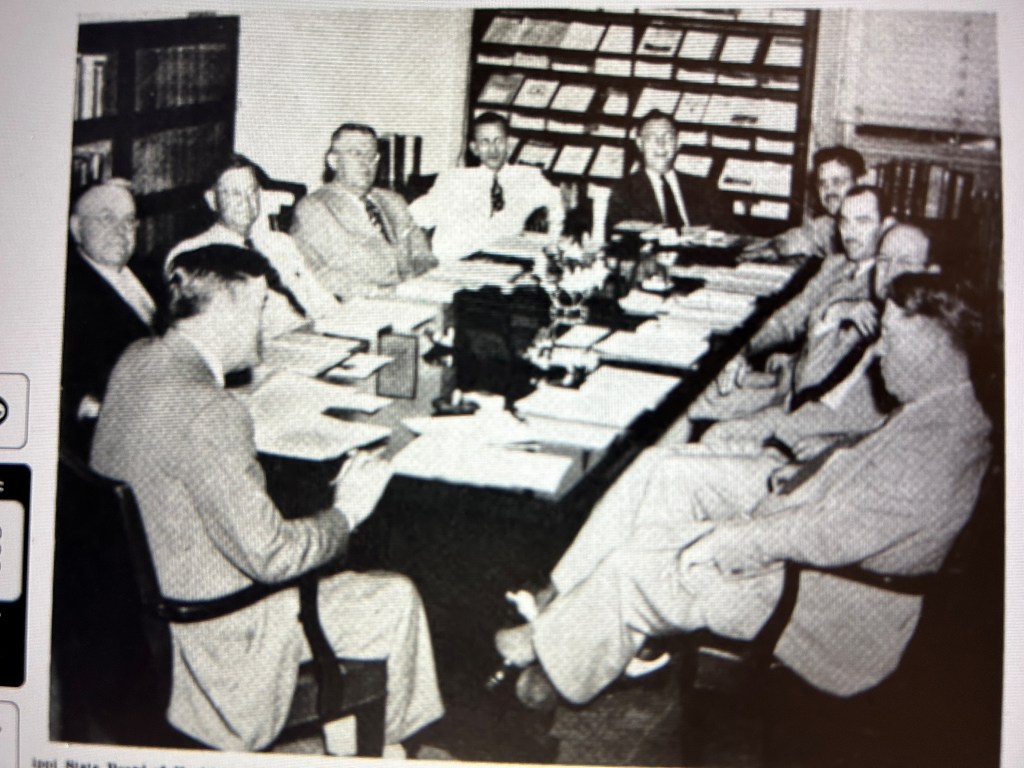
A ten member Mississippi Board of Health wrote and administered their state’s licensing exam. The twelve subject areas covered on the exam during the 1924=1958 period are listed here.
Anatomy* Physiology* Hygiene* Obstetrics* and Gynecology Surgery* Pathology* Histology/Bacteriology Chemistry* Diseases of eye, ear, nose, throat Materia Medica* Theory and Practice of Medicine Physical Diagnosis
*indicates original subject areas called for in the 1882 legislation
Individual members of the Mississippi Board wrote six to ten questions for their assigned subject area. All questions were constructed as “open” or extended response items. There were no multiple-choice questions (MCQs) on the Mississippi exam during this period. This is hardly surprising. MCQs did not feature prominently on any state exams for medical licensure or on the National Board of Medical Examiners Parts exam until the 1950s.
Absent information to the contrary, it is presumed that the board member writing the questions for a subject area also carried the responsibility for scoring those items.
I have found no detailed information on the scoring scales or requirements specific to achieving an overall passing level performance on this exam. The 1882 law called only for candidates to present an examination that “prove[d] satisfactory” to the Board.1 As late as 1947, the law only referred to the examination results providing evidence of “sufficient learning.”2 The various volumes donated by the Mississippi board to the FHC do not present any specific information on the scoring. Thus, we don’t know the answer to a few basic questions: Did the Board require a passing score on each individual subject area in order to achieve an overall passing outcome? Or were subject area scores rolled up into an aggregate score with its own specified minimum for passing? (Note: States commonly specified 75 in their state statute as the minimum pass.)
Exam performance data
So how tough was this Mississippi exam? To answer this question, I leveraged the data collected and published annually in JAMA as “State Board Statistics” (1924-1929) and subsequently retitled as “Medical Licensure Statistics” (1930-1958).
For the 35-year period spanning the years 1924-1958, a grand total of 1,768 individuals were examined by the Mississippi Board—an average of 50 candidates per year. And the results? We are definitely not talking about the Bataan death march of assessment. All but 23 candidates passed the exam—a 1.3% fail rate for this entire period! (See the Appendix 1 below)
From a purely statistical perspective, this exam presented a minor hurdle for the vast majority of candidates. Indeed, in twenty-three of the 35 years of this study no candidates failed the exam in Mississippi. Though this may seem surprising it was actually not uncommon based upon the reported performance outcomes on other states’ medical licensing exams. Looking nationally at the period 1924-1958, twenty-three states reported years in which no candidates failed their medical licensing exam. Thus, Mississippi’s modest 1.3% overall fail rate ranks 25th (median) among all states during this period. (see Appendix 2)
Interestingly, this was definitely not the case previously on the Mississippi exam. Only a decade earlier, the fail rate on Mississippi’s exam fell on the other end of the spectrum. The first 5-year period reported by JAMA showed Mississippi with the highest failure rate on its exam compared to all other states.
Years
# MS candidates
% failed
National rank
1908-1912
1,172
55%
1st
1914-1918
284
23%
11th
1919-1924
124
8%
25th
A dramatic swing involving the Mississippi exam took place sometime around the start of World War I. What happened precisely is unclear but we can speculate on reasons for both the sharp drop-off in number of candidates being examined by Mississippi after 1912 as well as the steady decline in their fail rate.
In terms of the volume drop off, prospective licensees may have begun avoiding Mississippi because of the high fail rate on its exam which would have been publicly known through JAMA’s annual publication of state specific exam results. It is also possible that changes to state law or board policy may have directed more incoming physicians from other jurisdictions into licensure by reciprocity or endorsement scenarios that allowed them to bypass the exam. Perhaps the strongest factor in the declining numbers and also the fail rate was the change to state law in 1919 that required licensure candidates to be graduates of Class A school2 under the AMA Council on Medical Education’s classification system.
It also bears mention that Mississippi had one of the lowest physician-to-population ratios in the United States at 1:1640. Board Chair Felix Underwood called it the “most serious and complex public health problem” in the state’s history.3 With the Mississippi Board keenly aware of this shortage, I can’t help but wonder if this worked at least unconsciously on the Board’s vetting of physician candidates and even its scoring of candidates’ exams. See Appendix 3
By 1914 and through the start of World War II, the number of physician candidates examined by the Board stabilized at a modest twenty to thirty annually in most years with a fail rate hovering around 2%.
Mississippi board composition and impact on the exam
The ten-member Mississippi board wrote and administered its medical licensing examination. Board members served six-year staggered terms. Assuming scoring was done by a single board member for each subject area, changes to board composition directly impacted both the exam’s content and its scoring.
Thirty-five (35) individuals served on the Mississippi board during the period 1924 to 1958. The mean length of service was nearly a decade (9.57 years) with a dozen individuals serving 12 or more years on the MS board. Board Secretary Felix Underwood served 34 years, nearly the entire span of the time period under review. See Appendix 1
Paying attention to the Board’s composition is more than just historical minutiae. With an extended-response item format, the individuals making decisions about the correctness and sufficiency of the answers (i.e., the rater) represents the key factor impacting scoring and overall pass rates on the Mississippi exam. The information available to us does allow for analysis concerning how the number of raters scoring each subject area impacted potential scoring (in)consistency.
While two subject areas (Histology/Bacteriology and OB/GYN) had higher potential consistency by virtue of the small number of board members scoring those areas during this period, most subject areas had 3-4 different board members scoring that component of the exam from 1924-1958. Two areas (surgery, EENT) had probably the greatest potential for scoring variability.
Subject area
# scorers
Subject area
# scorers
Histology/Bacteriology
1
Pathology
4
OB/GYN
2
Physical Diagnosis
4
Anatomy
3
Theory & practice of medicine
4
Hygiene
3
Materia Medica
5
Physiology
4
Surgery
7
Chemistry
4
Diseases of eye, ear, nose, throat
7
We might think that a single examiner scoring a subject area over the entire period is the ideal. While such was the case for histology/ bacteriology, the practical reality is that the time-period in question is so long that there were likely multiple changes over time impacting the judgment of a sole rater on an biannual test administration. For instance, rater tendencies and predilections involving specific focus or emphasis in crafting questions within the subject area; changing expectations of what constitutes an acceptable minimum level of performance by a candidate, etc. In other words, how a rater approached both what questions to ask and how they should be scored ultimately shift over time even when only a single rater was involved in a subject area. As one scholar put it, “assigning a grade to an essay is not a precise science.”4 This is not conjecture. Ample evidence exists in the scholarly and technical literature specific to scoring extended response items demonstrating that rater (in)consistency is highly problematic to exam reliability.
At the same time, it seems unlikely that the rater composition, regardless of (in)stability, had much impact on licensure candidates in Mississippi. Why? Going back to the performance data, few individuals (n=23) failed to demonstrate adequate knowledge to that board. The examination in Mississippi presented an easily surmounted hurdle in the candidate’s journey to licensure.
So was the medical licensing exam in Mississippi little more than pro forma ritual? A performative exercise for gaining admittance to the profession? Perhaps. But in order to answer this we have to look directly at the questions being posed on the Mississippi examination. How relevant were they? Were they quality items allowing the rater to glean insights into the knowledge and competence of these candidates? For this, we sought subject matter review. That will be subject of my next blog post.
To be continued….
The opinions expressed are those of the author and do not represent the views of the Federation of State Medical Boards.
Endnotes
See Section 17 of An Act to Regulate the Practice of Medicine in the State of Mississippi (Jackson: State Printer, 1882).
Mississippi Laws and Extracts of Laws Dealing with Public Health (Jackson: Mississippi State Board of Health, 1947), 104
Lucie Robertson Bridgforth, “Politics of Public Health Reform,” The Public Historian, 1984, p. 19
Gavin T. L. Brown, “The Reliability of Essay Scores: The Necessity of Rubrics and Moderation,” in Tertiary Assessment and Higher Education Student Outcomes: Policy, Practice and Research. Ed. Luanna H. Meyer, et. al. 2009
Appendix 1
All candidates for Mississippi examination
Year
Total
# pass
# fail
Fail %
MS fail % compared to nat’l
# states w/ 0% fail
1924
21
20
1
4.7%
21st
28
1925
28
28
0
0%
24th
27
1926
20
18
2
10%
5th
25
1927
21
21
0
0%
35th
16
1928
24
24
0
0%
32nd
19
1929
27
27
0
0%
30th
21
1930
33
31
2
6.0%
10th
27
1931
35
35
0
0%
25th
26
1932
27
27
0
0%
25th
26
1933
24
24
0
0%
26th
25
1934
29
28
1
3.4%
14th
22
1935
31
30
1
3.2%
16th
19
1936
26
22
4
15.3%
8th
26
1937
18
22
2
9.0%
14th
18
1938
32
31
1
3.1%
16th
21
1939
22
22
0
0%
25th
26
1940
42
42
0
0%
28th
23
1941
38
38
0
0%
27th
24
1942
45
43
2
4.4%
14th
24
1943
114
113
1
0.9%
23rd
22
1944
60
60
0
0%
24th
27
1945
50
50
0
0%
25th
26
1946
45
45
0
0%
28th
23
1947
59
59
0
0%
22nd
29
1948
47
47
0
0%
27th
24
1949
40
35
5
12.5%
7th
19
1950
64
63
1
1.5%
22nd
21
1951
77
77
0
0%
28th
23
1952
83
83
0
0%
27th
24
1953
84
84
0
0%
25th
26
1954
80
80
0
0%
27th
24
1955
75
75
0
0%
33rd
18
1956
101
101
0
0%
32nd
19
1957
122
122
0
0%
34th
17
1958
124
124
0
0%
26th
25
Total
1,768
1,745
23
1.30%
Mean 20th
Mean 23
Median 25th
Median 24
Mode 25th
Mode 26
Source: Compiled from JAMA “State Board Statistics” (1924-1929) and “Medical Licensure Statistics” (1930-1958). This appeared annually—usually in April or May.
Appendix 2
# of Physicians in MS, 1938-1947
Year
Total
White
“Colored”
1938
1446
1392
54
1939
1436
1381
55
1940
1425
1372
53
1941
1356
1306
50
1942
1330
1279
51
1943
1200
1151
49
1944
1160
1111
49
1945
1112
1060
52
1946
1213
1163
50
1947
1351
1298
53
319 MS physicians served in WWII
Source: Public Health and Medical Licensure in Mississippi, Vol 2. FJ Underwood, RN Whitfield. Jackson: Tucker Printing House, 1938, p. 378
Appendix 3
Mississippi Board members 1924-1958
Board member
Years serving
Total # Yrs
Subject area
Arrington
1958
1
pathology
Austin
1924-1943
20
Anatomy; Materia medica
Avent
1947-1958
12
Chemistry
Banks
1934-1957
24
Pathology
Blackburn
1950-1958
9
Hygiene
Brock
1936-1941
6
Physiology
Brown
1925
1
Material medica
Caldwell
1944-1958
15
EENT; Surgery
Crawford
1926-1929
4
Surgery
Culpepper
1942-1947
6
Physical diagnosis
Dampeer
1924-1929
6
Physiology
Darrington
1931-1935
5
Surgery
Dearman
1931-1935
5
Physical diagnosis
Eason
1924-1951
18
OBGYN
Field
1942-1958
17
Physiology; Materia medica
Frizell
1930-1935
6
Physiology
Gamble
1944-1956
13
Anatomy
Garrison
1948-1958
11
Theory, practice of medicine
Gavin
1924-1925`
2
Hygiene
Haralson
1924-1925
2
Pathology
Holmes
1925-1927
3
Chemistry
Hooper
1924
1
Chemistry
House
1952-1958
7
OBGYN
Howell
1936-1941
6
Surgery
Lipscomb
1926-1943
18
Theory, practice of medicine
Long
1942-1948
7
Surgery
McKinnon
1936-1941, 1948-1958
17
EENT, Physical diagnosis
Seale
1925
1
Theory practice of medicine
Shaw
1928-1946
19
Stennis
1926-1933
7
Pathology
Underwood
1925-1958
34
Histology/bacteriology
Wall
1924-1925
2
Surgery
Watson
1926-1929
4
EENT
Wilkins
1957-1958
2
Anatomy
Wright
1926-1949
24
Hygiene
35 members
Average length of service in years: Mean 9.57 Median 6 Mode 6
Source: Two-volume set of Mississippi Board of Health licensing exam questions housed at the FSMB Historical Collection
We know a good deal about the early history and development of our system for medical licensure in this country. Historian of medicine Richard Shryock and medical regulator Robert Derbyshire1 contributed short but valuable works in the 1960s. Sociologist Paul Starr addressed licensing as one part of his masterwork on the social development on the medical profession.2 Scholars like Ronald Hamowy and Samuel Baker authored oft-cited journal articles looking specifically at the legislative origins and evolution of early medical licensure3 while the historian James Mohr explored the legal basis for medical regulation.4 What all of these authors contributed were broad brush stroke portraits of our medical licensure system—narratives delivering a valuable macro-level view of the subject.
What has been less frequently presented are state-level analyses of these origin stories for medical licensure. A scholarly few exist: Clinton Sandvick for Illinois, Samuel Baker for Massachusetts. Yet there is little in the scholarly literature that takes even a cursory look at the demographic profile of early licensees in any state. To put it bluntly, we have seldom posed the question, “Who were these guys?” (And yes, I know there were women too; small in number attempting to succeed in an entrenched patriarchal landscape)
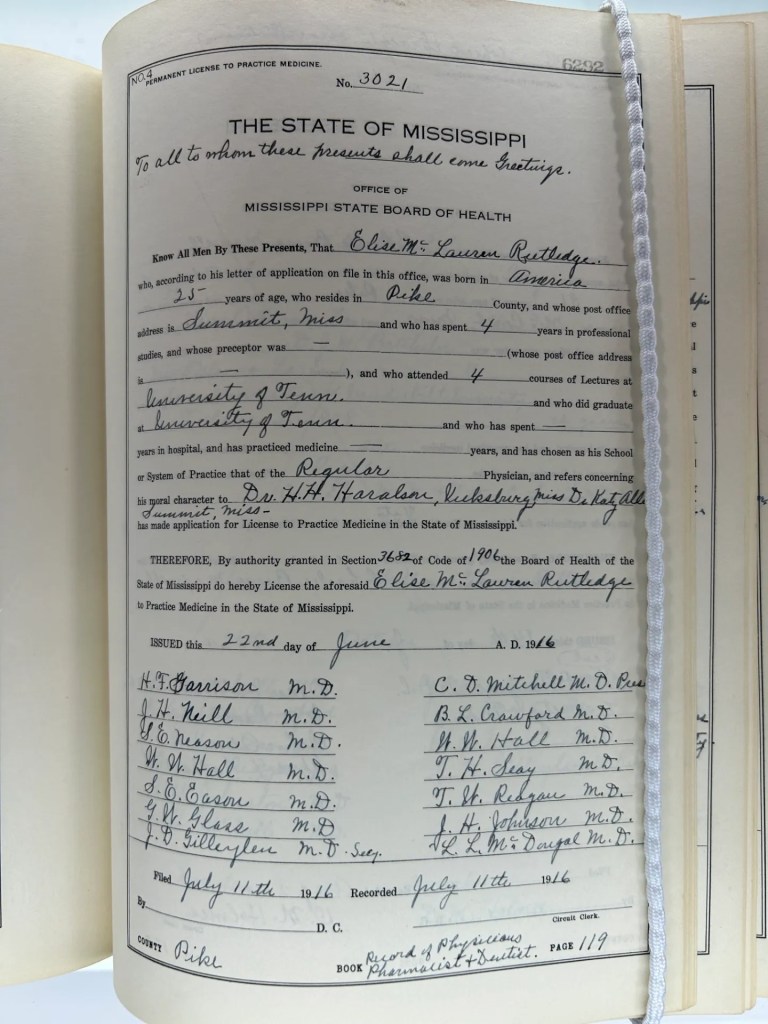
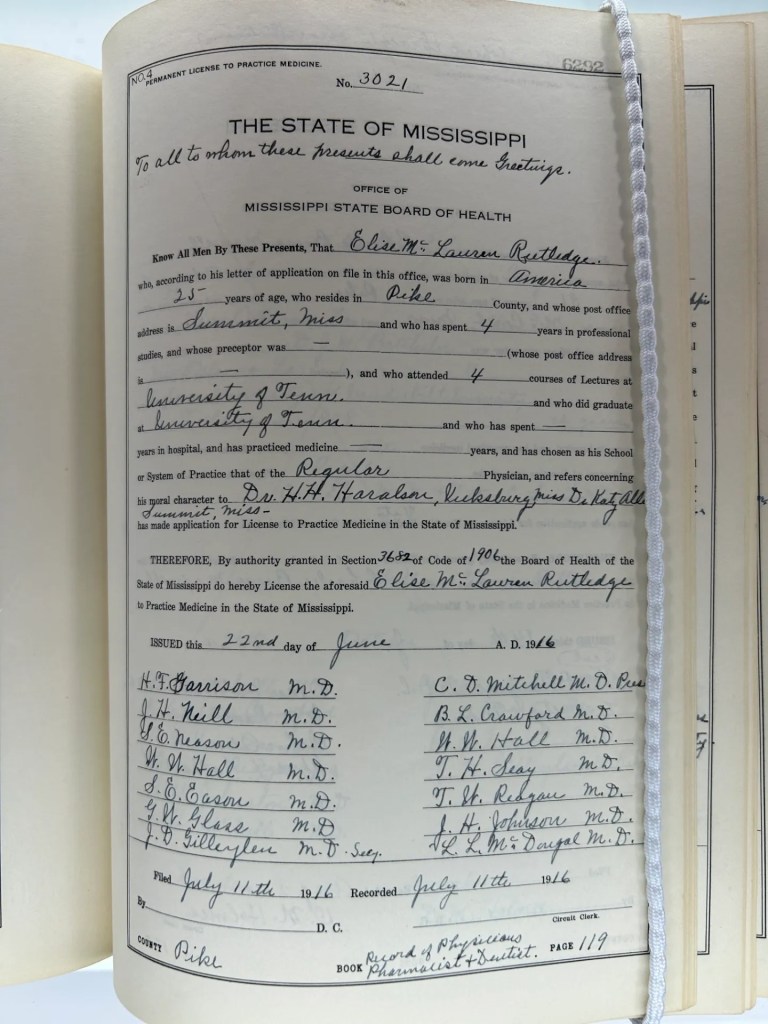
The gift of a series of registry books from the Mississippi State Board of Medical Licensure to the FSMB Historical Collection provided me with an opportunity to explore that ‘Who were they?’ question directly. The donated volumes contained thousands of individual records assembled as part of a 1930s W.P.A. project for the Mississippi Department of Health—specifically individual applications for medical licensure in that state.
The time available to me precluded reviewing the entirety of the records contained in those volumes. Instead, I undertook a targeted, hopefully representative sampling from those volumes—approximately 472 records. What follows is a demographic summary of that sample set supplying insight into the early licensed practice of medicine in Mississippi. Who were they? Where were they educated? How much (in)formal training did they bring to their practice?
The 472 individuals were licensed over six decades (1882-1940). The majority of the records (80%) fell within the first three decades of that period. It comes as no surprise that the licensees over overwhelmingly male over this time span. Only six women were found to have been licensed in this sampling. Similarly, this sample found only four likely black physicians if we infer race from their associated medical school (Meharry-one of the historical black medical colleges).
While intra-professional strife characterized the relations between “regular” (i.e., allopathic) physicians and their “irregular” brethren for the second half of the nineteenth century, the small number of non-allopaths during this extended period (n=15) suggests these tensions may have minor irritants at best in Mississippi. The fifteen were categorized by the board as either eclectic, homeopathic, botanic or mineral physicians. Interestingly, no osteopathic physicians appeared in this data set spanning six decades.
Time period
# of licensees
Holds Medical degree
Preceptorship
“Irregular” practitioners
1882-1890
172
68 (39%)
125 (73%)
15
1891-1900
79
48 (61%)
41 (52%)
0
1901-1910
126
60 (47%)
57 (45%)
0
1911-1920
41
34 (83%)
2
1
1921-1930
35
34 (97%)
3
0
1931-1940
19
16 (84%)
0
0
Total 1882-1940
N=472
N=260 (55%)
N=228 (48%)
N=16 (3%)
One question peaking my curiosity involved education—what type of medical education and training did these early licensed physicians bring to the treatment of their patients in Mississippi?
Only 55% of all the physicians in this sample reported having graduated with a medical degree. For those who did, where they attended medical school is worth sharing. Few of these physicians obtained their medical education and degree outside of the South. The medical colleges in Tulane and Memphis were the primary source institutions with 116 and 115 licensees respectively. Degree holders from schools in Louisville, Nashville and Jackson were smaller in number but still significant sources of the degreed-physicians in Mississippi.
Only 15 of these licensees presenting a medical degree obtained that credential from an institution outside of the South. Schools in Chicago, Cincinnati, New York City and Philadelphia predominated. (Note: My definition of the “South” included border states such as Missouri, Kentucky, Maryland)
If the strong southern orientation of the medical schools for these degree holding physicians didn’t surprise me, something else did: The number of individuals reporting medical education from more than one institution. More than one quarter (n=128) of the 472 physicians in the sample reported attending lectures at two or more medical colleges. While speculative, it may be surmised that repeating a set of didactic lectures at a second school was, if not common, then at least not unusual. Additionally, seeking clinical experience away from the school providing the core medical lectures seems understandable in an era when the onus for obtaining training fell more to the physician rather than their institution.
One of the more telling figures in suggesting the profoundly different educational landscape for medicine at that time involves the number of licensees presenting to the Mississippi board absent a medical degree. Less than half (46%) contained in this sample covering the period 1882-1910 possessed a medical degree.
This may seem strange to us today. However, like many states, the introduction of licensure laws in Mississippi included provision for licensing individuals who did not attend or graduate from a medical college.5 The reality is that such provisions were pragmatic in nature as state legislatures opted more often than not to grandfather in those individuals already practicing in the state who might not otherwise meet newly implemented requirements.
A total of 212 individuals reported no medical degree…and yet all but 27 of these physicians reported having attended at least one set of lectures at a medical college. Thus, licensed physicians who were wholly self-taught or trained solely via preceptor or apprentice relationships constituted only 6% of all the licensees in this sample.
The most common experience among the Mississippi licensees spanning these first three decades involved preceptorship. 59% of all the licensees during that period claimed one. Interestingly, familial connections may have played a prominent role in this as 55 of the 223 licensees did their preceptorship with a physician bearing the same last name. While some of these may have been coincidence, it seems likely that familial connection (father, brother, uncle, cousin) facilitated the training. The reported length of time under preceptorship seems not insignificant—a 3-years mean/median across the entirety of the sampling. Even if this self-reported data is inflated by half, it suggests that informal training occurred longer and more extensively than one might have thought.
One caveat to the preceptor data. This practice was common enough that it remained a standard field on the licensing application throughout the entire 1882-1940 time period. However, it was clear to me that some physicians (or the staff member filling in the form) classified the clinical portion of their medical education under the preceptor category. I excluded those instances where it seems clear this was being done.
So what to make of this data? Perhaps the key word to keep in mind is dynamic. This data, while specific to a single state, reflects the evolving nature of the medical educational and regulatory systems in late nineteenth and early twentieth century America—essentially a system in flux. Educational standards were still being formulated through a de facto accreditation process via the AMA Council on Medical Education and AAMC. Legislatures were following that lead by codifying these classifications for medical schools as the basis for licensure: Graduates of Class A and B schools as eligible; Class C graduates ineligible. Mississippi required graduation from a Class A school starting in 1919.6 Legislatures enacted and medical boards operationalized licensure requirements mindful of this still evolving educational landscape as well as the presence of thousands of established practitioners whose medical careers predated these changes.
Of course, we should be cautious in drawing conclusions from what is a sample set of data. Still, the data is consistent with what we would expect during a transition era in the history of the profession and the regulatory system. Perhaps an ambitious scholar would like to visit the FSMB Historical Collection and use these records for a more systematic survey and analysis?
The opinions expressed are those of the author and do not represent the views of the Federation of State Medical Boards.
Richard Shyrock, Medical Licensing in America, 1650-1965 (Johns Hopkins, 1967); Robert Derbyshire, Medical Licensure and Discipline in the United States (Johns Hopkins, 1969)
Paul Starr, The Social Transformation of American Medicine (Basic Books, 1982)
Ronald Hamowy, “The Early Development of Medical Licensing Laws in the United States, 1875-1900,” Journal of Libertarian Studies, 1979; Samuel Baker, “Physician Licensure Laws in the United States, 1865-1915,” Journal of History of Medicine and Allied Sciences, 1984
James Mohr, Licensed to Practice (Johns Hopkins, 2013)
See Section 17 of An Act to Regulate the Practice of Medicine in the State of Mississippi (Jackson: State Printer, 1882)
Mississippi Laws and Extracts of Laws Dealing with Public Health (Jackson: Mississippi State Board of Health, 1947), 104
The rich history of medical regulation in the United States spans one hundred and fifty years. Since its centennial in 2012, the Federation of State Medical Boards has been collating and cataloging its various archival materials and holdings and seeking additional materials capturing the rich history of state medical boards.
In 2021, FSMB President Hank Chaudhry, DO, encouraged staff to create a permanent physical space in the organization’s Texas offices for sharing the story of FSMB and the state medical board community. I have been honored to lead this initiative.
On October 24, 2024, the Federation of State Medical Boards held a grand opening for the FSMB Historical Collection (FHC). This event showcased the culmination of many years work to gather, assemble and curate the materials featured in the FHC.
So what is the FSMB Historical Collection (FHC)? The FHC comprises a multi-purpose space integrating a library, archive and display materials. The FHC houses contemporary and historical scholarship on various aspects of medical regulation, education, assessment and the growth of the medical profession. Its archival holdings include documents and photographs spanning the entirety of the FSMB’s 113-year history. The assembled artifacts and interactive touchscreen displays provide visitors with a glimpse into FSMB’s history and various aspects of medical regulation such as our current displays on medical discipline, the licensing examination and prominent women in medical regulation.
To give a flavor for the FHC’s holdings, here are a couple items I wanted to spotlight.
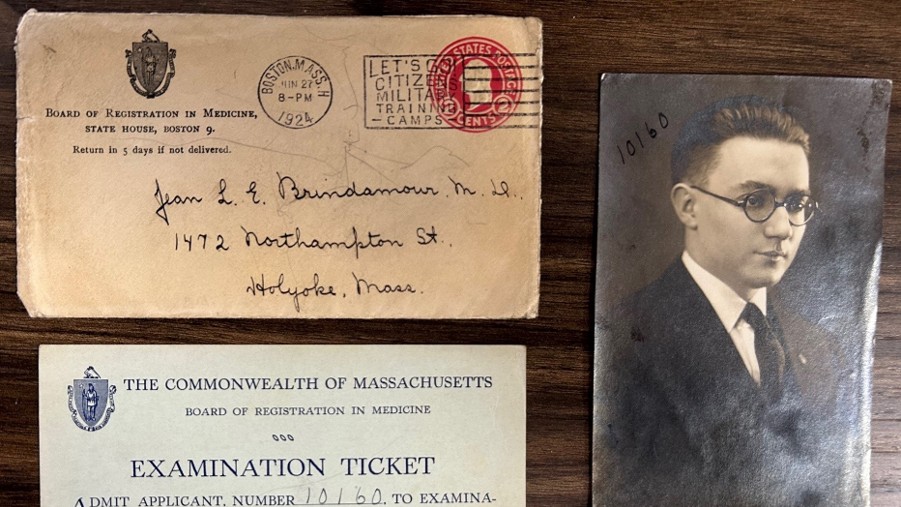
For many decades, the primary function of state medical boards included writing, administering and scoring a medical licensing exam for prospective licensees in their state. Very little seems to have survived showcasing the administrative features of these exams. That’s what makes these items from a 1923 examinee to the Massachusetts medical board’s exam so fascinating.
Among the other exam related materials at the FHC are these test prep books from various publishers during the first half of the twentieth century. Medical licensing exams were almost exclusively extended response questions. A common practice called for post-administration publishing of the board’s test questions. This occurred in either a publication of the board, a state medical society journal or even JAMA. The rationale was simple: publishing previously used questions gave prospective examinees some idea for how to prepare for the exam. Publishers soon recognized the market for gathering and publishing these questions dispersed in various journals across the country. The modern equivalent is Kaplan, First Aid for USMLE, UWorld, etc.
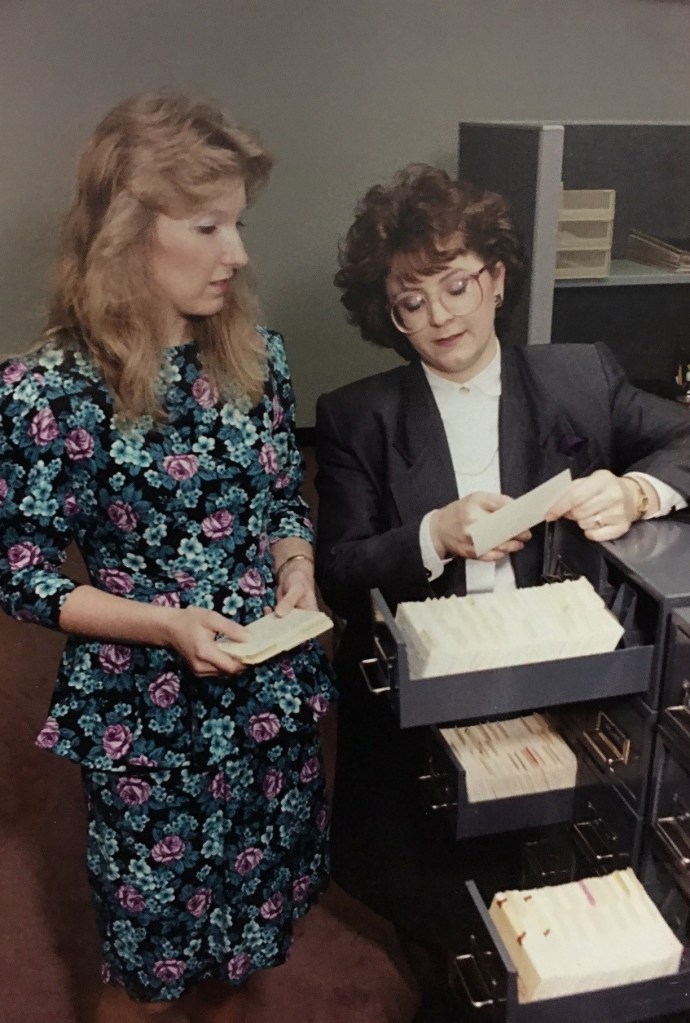
One of my favorite items in the collection is this industrial looking card catalog.
Once the FSMB secured permanent offices in Texas in 1962, it began receiving notices of disciplinary actions taken by state medical boards across the country. The FSMB’s modern Physician Data Center has its modest origins in this card catalog holding summaries of disciplinary actions dating to the early 1960s.
A generous donation from the Mississippi State Board of Medical Licensure serves as a main exhibit today at the FHC. That board’s executive director has shared two sets of original materials. (1) Bound register books containing the license applications dating back to the 1890s. (2) A multi-volume bound set containing all the questions posed on the Mississippi exam from 1923-1968. Both sets make for fascinating reading. Both present a unique research opportunity for scholars.
Finally, if you are reading this post and have materials that touch upon the history of medical regulation and wish to contribute to the FHC (through donation or loan), don’t hesitate to contact me. We would love the opportunity to spotlight your historical artifacts.
The opinions expressed are those of the author and do not represent the views of the Federation of State Medical Boards.
Earlier this summer my wife and I were traveling through Colorado and spent a couple nights in Trinidad. After a nice dinner at a Mexican restaurant in their downtown, we strolled the streets, window shopping and enjoying the mild weather. We ran across a placard inside one building that gave a bit of history to that site and Trinidad’s early days.
The placard related a number of “firsts” dating to 1867, including mention of Dr. Michael Beshoar as the proprietor of the “only drug store Santa Fe to Denver.”
I was taken aback when I read the name. Michael Beshoar didn’t just ring a bell. I knew precisely who he was and why I remembered that name. It turns out that one of Trinidad’s most famous early physicians had a direct connection to America’s largest medical diploma mill. As Dr. Beshoar learned firsthand, eighteen hundred miles wasn’t far enough to distance himself from a questionable decision and even more dubious connection.
Prior to seeing Beshoar identified as a prominent early citizen of Trinidad, my knowledge of him derived from familiarity with seeing his name on the printed list of faculty for John Buchanan’s medical college in the mid-1870s. I learned a bit more about Beshoar when I discovered the Denver Public Library contained archival materials including his “papers.” From these I learned that Beshoar’s connection with the infamous diploma mill dated to 1873.
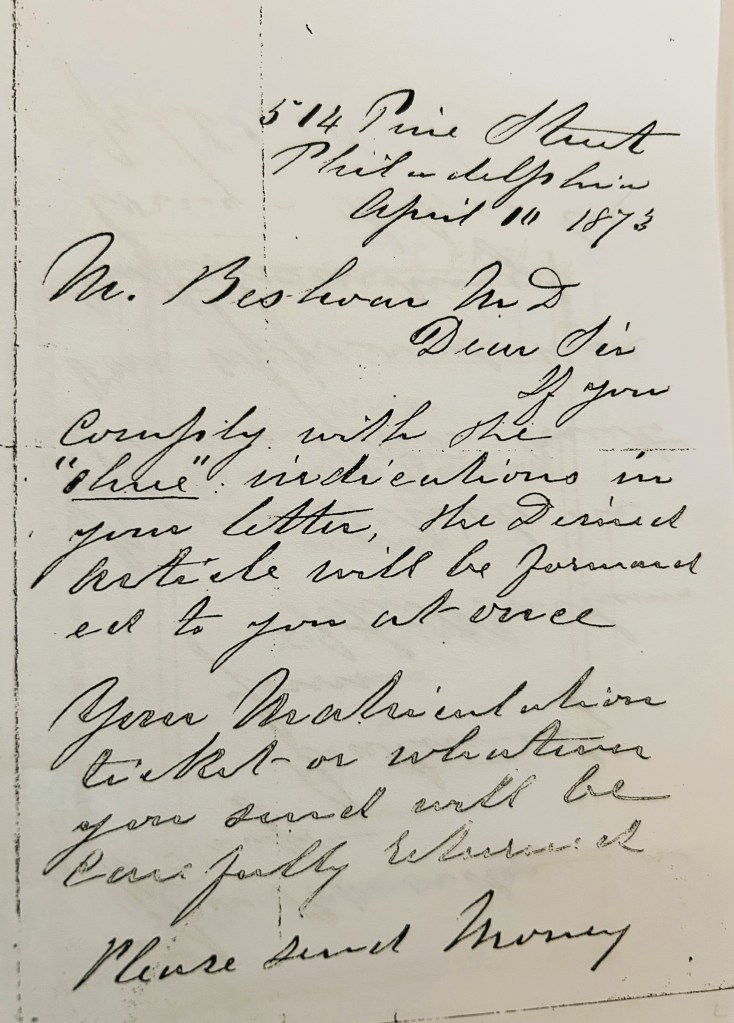
On April 10 of that year, John Buchanan responded to an inquiry from Beshoar stating:
“Dear Sir, if you comply with the [?] directions in your letter, the desired article will be forwarded to you at once. Your matriculation ticket or whatever you send will be carefully [?]. Please send money for P.O. order or draft.”
The indirect language and euphemism (“desired article”) were common features of John Buchanan’s operative style when dealing with prospective customers by mail. The context for this letter and later exchanges between the two men make it clear that Beshoar had expressed interest in purchasing a diploma from one of Buchanan’s legally chartered schools: the Eclectic Medical College (EMC) or the American University of Philadelphia.
Another letter from 1879 included an interesting pledge from Buchanan. He assured Beshoar that, “we shall take care of your interests if there is any inquiries.” Whether this was specific to securing students for his fall 1879 classes at the EMC or if this alluded to the press inquiries growing more frequent concerning the nature of Buchanan’s operations is unclear. One suspects that Buchanan stood behind both.
When I finished my book on the subject (Diploma Mill), my view of Dr. Michael Beshoar was uncomplicated. He was simply one of the rogues unmasked by the Philadelphia Record’s crusading editor, John Norris after authorities’ arrest and search of Buchanan’s offices at 514 Pine Street. But that placard in Trinidad gave me pause. What did I really know about Dr. Beshoar? Was he just another of Buchanan’s scoundrels? Or was there more to his story?
I decided to look more closely. As you’ll see, the picture becomes more nuanced and less clear. (Note: The same is true for another EMC “graduate” that I wrote about in 2019)
Michael Beshoar was born in 1833 and later graduated from the University of Michigan’s medical college in 1853. Beshoar relocated to Arkansas where he established deep roots: he married, established a medical practice and served in the state legislature. When the Civil War broke out, he served as a medical officer for the Confederacy. Captured in 1863, he began treating Union troops and ultimately served the U.S. Army at Fort Kearney in Nebraska Territory.
A flamboyant frontier persona
By 1867, he drifted into Colorado, first Pueblo and then Trinidad. In the latter town, his wide interests and boundless energy saw him practicing medicine, operating a drug store, creating his own patent medicines; and later opening a newspaper, engaging in land speculation, serving on a vigilance committee, pursuing local and state political offices and much more. Dr. Michael Beshoar’s boundless energy and entrepreneurial interests touched just about everything and everyone in the Trinidad region.
All of which begs the question: Why did Michael Beshoar get mixed up with America’s most notorious medical diploma mill?
To understand this, we need to go back to Beshoar’s days in Arkansas. Like so many Southerners, the Civil War ruined him financially. In an 1879 letter, he claimed to have come out of the war with “$1.20 suit of summer clothes” and little else. Thousands of acres that he had procured earlier in northern Arkansas were lost to back taxes. His dreams (“I was sure to being a millionaire in a few years”) were dashed.
Still, ambition never seemed to wane in Beshoar. While he studied and practiced medicine, Beshoar appeared to see himself as much more than just a physician. Ambition is the key to understanding Dr. Michael Beshoar and ultimately his interactions with Dr. John Buchanan.
Let’s go back to that 1873 correspondence with John Buchanan. At that time, medicine was effectively an unregulated field in this country. Only North Carolina and Texas had laws in place controlling medical practice. Even then I doubt whether much, if any, enforcement of these laws took place.
Most Americans’ experience of health care involved what we would categorize today as folk medicine, i.e., botanical remedies delivered in the home by family, friend or a trusted neighbor. The “doctor” called in to render aid was more often a local healer whose skills (real or perceived) were valued in their own right. Probably only a minority of Americans received treatment at the hands of a doctor as defined by someone possessing a medical degree or diploma.
Recall that Beshoar received a medical diploma from Michigan. So why would he have been seeking one of Buchanan’s diplomas? Initially, I thought the likely explanation was simply that Beshoar no longer had the sheepskin credential in his possession after his many moves. That turned out not to be the case as newspapers covered Beshoar’s attendance at a 1903 reunion in Ann Arbor where he produced the original diploma and seal issued to him half a century earlier.
So if it wasn’t a case of replacing a lost diploma, why would have wanted one from Buchanan? The answer may be as simple as this: While a medical degree wasn’t necessary to practice in Colorado, it was a great distinguisher that could only enhance Beshoar’s standing in the community. So, if he was going to have a diploma, it couldn’t hurt to have a degree from a school in Philadelphia, the unchallenged epicenter of American medicine. Beshoar’s would have been an ad eundem degree, i.e. one conferred in addition to an earlier degree. This is entirely speculative on my part but wholly plausible. This was a fairly common practice among 19th century colleges and universities.
Beshoar and Buchanan engaged in periodic correspondence in the 1870s. In his February 1875 letter to Beshoar, Buchanan wrote, “Your letter and proposition accepted….” Beshoar had apparently requested appointment to the EMC faculty and though the appointment ultimately was just titular (Beshoar’s name on the faculty list), their correspondence makes clear that Buchanan actually expected Beshoar to join him in Philadelphia to teach the fall 1875 session. Their correspondence continued into 1878 with Buchanan still hoping for Beshoar’s presence on-site and asking for a photograph so that all faculty could be represented in their advertising.
Ultimately, Beshoar did receive a Buchanan diploma and had his name on the faculty list presented in the EMC’s journal and the school prospectus. While these items might have been showcased in Beshoar’s office, they later proved problematic for him.
In the summer of 1880, John Buchanan was arrested and his offices searched. His subsequent faked suicide and flight from justice made front page news across the country. The Philadelphia Record and other newspapers printed various materials captured in the police raid, including exhaustive lists of the many recipients of Buchanan diplomas. Nestled among the the names: Michael Beshoar of Trinidad, Colorado
In an undated letter, the president of the Colorado State Medical Society demanded that Beshoar appear to answer multiple charges including questionable advertising, misrepresentations about his relationship to the ‘Rocky Mountain Medical Association’ and his status as “Emeritus Professor of the Practice of Medicine in the American University of Philadelphia—a notorious mill concern.”
Since the Colorado State Board of Medical Examiners wasn’t established until 1881 there were no licensing repercussions for Beshoar. And at the end of the day, membership in the state medical society wasn’t necessary to practice medicine.
So where did this leave Beshoar? Perhaps slightly embarrassed and the subject of snide comments from locals who heard the rumors coming from Beshoar’s medical brethren but probably not much more.
His interactions with Buchanan and his dubious medical colleges carried little risk for most of the 1870s. Beshoar sought a credential and a little gravitas through a titular faculty appointment that he likely saw as just a means to an end—bolstering his reputation and his medical practice in the community. These were precisely the moves of an energetic entrepreneur. Unfortunately for him, changing times brought legislation regulating the practice of medicine to every state and territory. The go-get’em spirit that rewarded bold, opportunistic types like Dr. Michael Beshoar looked a lot different by 1880 when the full nature of Buchanan’s diploma mill became known. Beshoar’s wide interests and influence in southern Colorado’s medical, political and newspaper communities made a fair number of rivals and outright enemies. His connection to Buchanan and the EMC provided easier fodder for critics looking to smear Beshoar’s reputation.
I have yet to run into anything in the historical record for Beshoar that suggests this blemish on his career made any lasting impression. While his grandson’s book, Hippocrates in a Red Vest, addressed the issue directly, his review of the evidence strongly suggests the links to Buchanan were a minor irritant in an otherwise remarkably diverse and successful career. Most of the sources and stories characterize him as a bit of free-spirited pioneer. Fair enough. Sleep well, Dr. Beshoar.
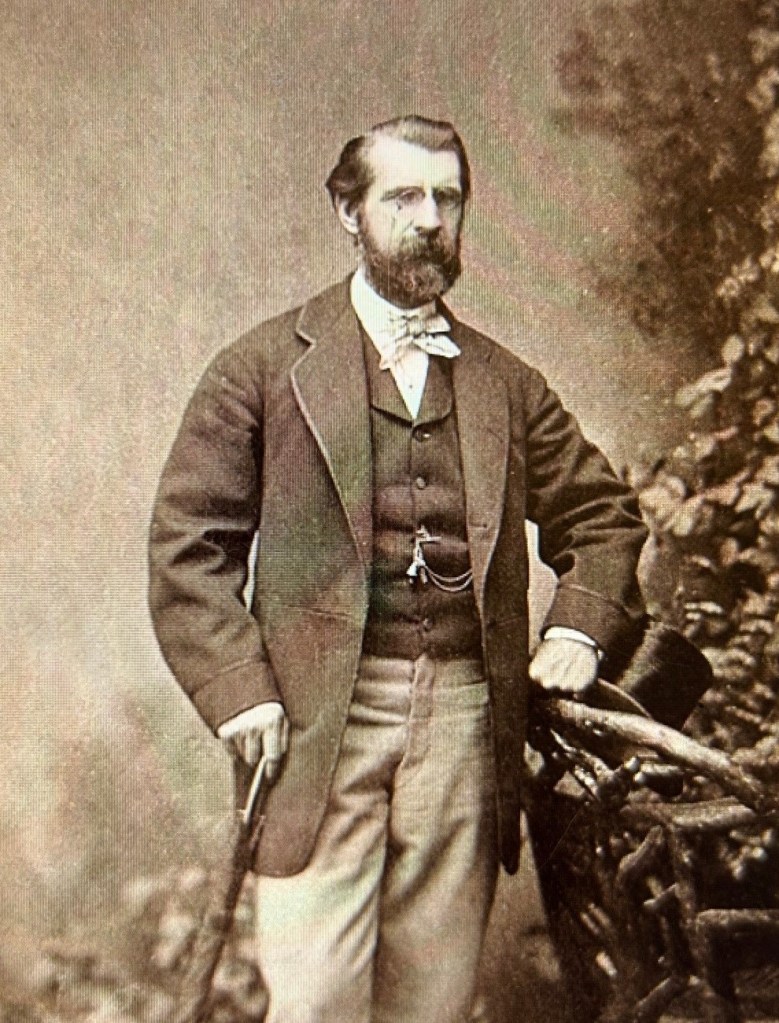
Dr. Beshoar in center right light colored top hat. Standing before one of the newspapers he founded.
The opinions expressed are those of the author and do not represent the views of the Federation of State Medical Boards.
Behind every U.S. Supreme Court case there is a human story. It is easy to lose sight of that truth behind the Latin phraseology and abstract legal doctrines. Sometimes the humanity involved springs to our mind just from the name of the case: Brown v. Board of Education of Topeka Kansas (1954), Griswold v. Connecticut (1965) or Loving v. Virginia (1967). It is impossible to think of these cases without contemplating lives and stories of Linda Brown, Estelle Griswold, Mildred and Richard Loving.
Last time on this blog I discussed the little known but important U.S. Supreme Court case, Hawker v. New York (1898). With the legal elements of the case covered in my last post, this time we’ll explore the unexpected human story behind this case.
I started by looking again at the text of the Supreme Court case that infamized Dr. Hawker. To my surprise in re-reading the case, I realized that the court never identified Hawker by his full name or offered any biographical detail. They referred to him solely as “plaintiff” or “defendant” depending upon his status in the chain of cases leading to the highest court. Several cursory Google searches for Hawker v. New York proved unavailing as virtually everything I saw simply looped back to the same non-specifics in the text of the court decision.
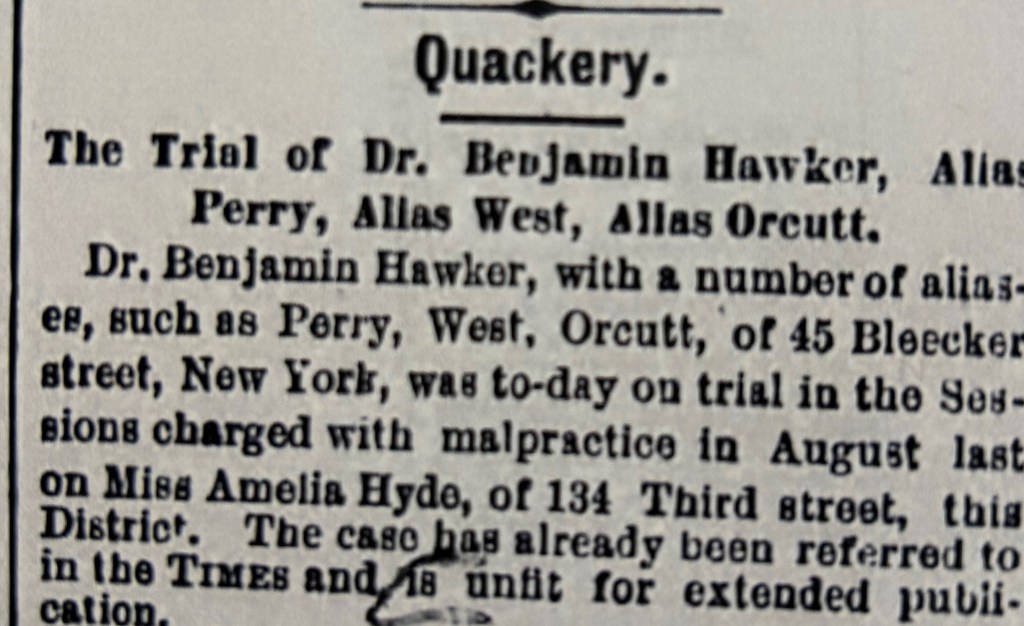
I tried another tact. I used my Newspapers.com account to search for news stories on Hawker. I searched first for items appearing in 1898 to see if I could learn his full name. Easy enough –Benjamin Hawker (New York Times, March 10, 1898, p. 10) Then I searched New York papers for the1878 trial and conviction that figured centrally in the Supreme Court case. Cue flood gates opening! As I quickly learned, Dr. Benjamin Hawker appeared in newspaper stories as early as 1871 and often thereafter until his death in 1903. Hawker’s medical practice can be traced definitively to 1870 in New York (though I suspect it began even earlier) and continued for decades under several names: Dr. Benjamin Hawker, alias Dr. West, alias Dr. Perry.
Benjamin Hawker practiced various names over the years–Perry, West, Orcutt.
(Note: To avoid confusing the reader, I will use the name Hawker throughout most of this post even when the cases involved his arrest as West or Perry)
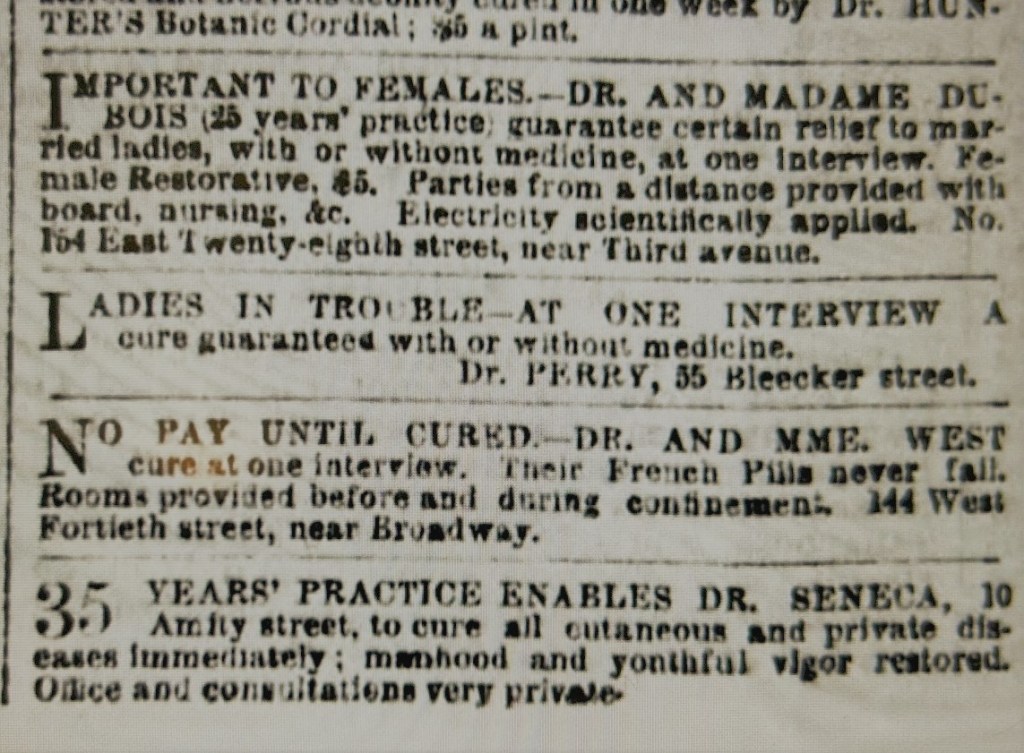
Piecing together Hawker’s personal history required a good deal of patience in wading through scores of news items. Most of these dealt with a series of medical disasters resulting from his services to “Ladies in Trouble” (his October 18,1870 ad in New York Daily Herald). If we exclude the legal cases leading to the 1898 Supreme Court decision, a total of four cases constituted the bulk of this press coverage over the years The death of Emily A. Post (1871), the death of Christina Brecht (1876) and a pair of 1877 medical malpractice cases involving Maggie McLoon and Amelia Hyde. Further notoriety for Hawker stemmed from his 1894 arrest as part of a major police operation that swept up sixteen “malpractitioners”; and, of course, his 1896 arrest for violating state law that culminated in Hawker v. New York two years later.
Newspaper ads like these were common; alerting potential customers to available services
As I parsed through all this material, I realized rather quickly that Benjamin Hawker was no medical innocent paying the price in 1896 for a single bad decision committed years earlier (1877). Nope. Hawker knew precisely the risks he took in the medical services he chose to provide. His eyes were wide open to the realities of medical jurisprudence in New York state…and he practiced accordingly as evidenced by his use of the Perry and West aliases.
So who was Benjamin Hawker? And where did he come from? How did he arrive at the practice of medicine in 1870? What kind of training did he receive?
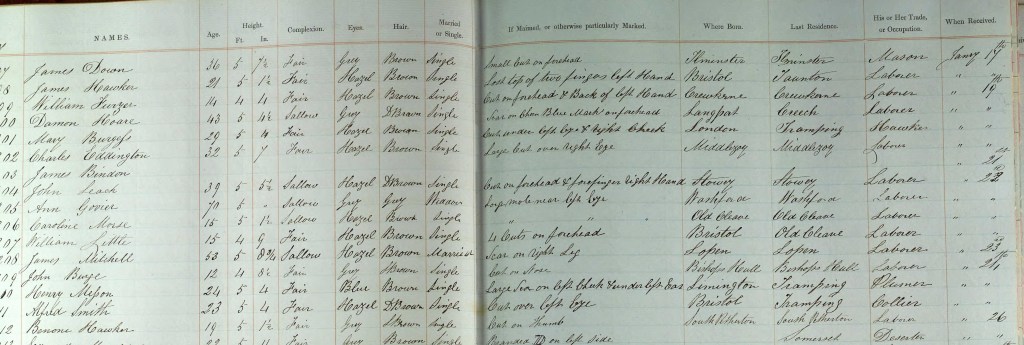
Hawker was born in December 1837 at Somerset, England, one of six children to Hugh Hawker and Ann Sibley. His given name at birth was Benoni, a name of Hebrew origin. (Benjamin was the commonly adopted Westernized version of Benoni) Two of his older brothers shared names with similarly strong Biblical ties: Jabez, Theophilos.
There is little else that can be said of Benjamin Hawker’s youth except that in 1857 he was committed to the Ilchester gaol in Somerset. His crime? Stealing two shillings from his employer which resulted in three months at “hard labor.”
Benoni Hawker is listed at the bottom in this page from Ilchester gaol register
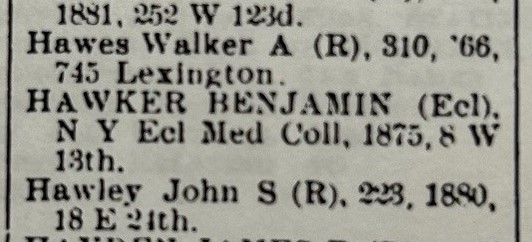
He arrived in the United States sometime in the 1860s. It is difficult to say when as a well-documented file in Ancestry.com identified an 1860 departure from England though Hawker later testified at an 1871 trial suggesting he arrived in the U.S. near the end of the Civil War. As part of that same testimony, Hawker claimed to hold a “certificate” from Guy’s Hospital (London) and to have been engaged in medicine for ten years. He acknowledged that he held no diploma though he asserted attendance at 2-3 medical courses. In 1876, he obtained a degree (or so he claimed) from New York Eclectic Medical College.
An 1890 physician register for New York. Hawker claims a medical degree here from 1875
It is difficult to know how much of Hawker’s statements we can accept as fact. For instance, in that same 1871 testimony he acknowledged that his last name wasn’t Perry (the name under which he practiced medicine). In fact, he claimed his name was Benjamin Arthur. Was this further obfuscation on his part? Abandoning one alias for another? Perhaps except that “Benoni Arthur” can be found in the 1870 federal census for New York city. Occupation? stencil maker.
It seems unlikely to me that Hawker practiced medicine as a means of support in the years immediately following his arrival in this country. He may well have survived as a stencil-maker; then again, we know that in October 1870 he was operating as Dr. Perry from his office at 55 Bleecker Street. Equally plausible is the possibility that “stencil maker” was nothing more than a convenient lie to the census taker. And the name “Arthur”? Well…perhaps that was his middle name or perhaps he just made it up, like stencil maker.
One thing is clear. Hawker kept offices on Bleecker Street throughout most of his career; and he often worked in conjunction with a female colleague. In the earliest years, this involved “Madame” Mary Van Buskirk; later this included Madame West, a woman named Mary Dunning or Gifford (accounts vary). His newspaper ads with the latter often stated that patients could “consult Dr. or Mme. West” at the Bleecker Street office.
Hawker’s first serious brush with the law as a physician occurred in 1871. Hawker and Van Buskirk’s efforts to terminate Emily Post’s late-stage pregnancy resulted in the death of both mother and child. The timing couldn’t have been worse for Hawker. His case overlapped with a lurid New York abortion death case, involving Dr. Jacob Rosenzweig (aka Dr. Asher) that captured national attention as the trunk murder mystery. In September 1871, a jury convicted Hawker of 4th degree manslaughter and applied the maximum sentence: two years imprisonment. In a separate trial, his colleague Madame Van Buskirk walked after a hung jury.
The case involving Emily Post’s death first brought Dr. Perry (aka Benjamin Hawker) before local authorities
By 1874, Hawker was out of jail and back in practice at his Bleecker Street address, Now, however, he practiced as Dr. West based upon his advertisements in the local papers. The death of one his patients, Christina Brecht, in February 1876 and her deathbed confession brought local authorities to Hawker’s office doorstep once again. Two elements are worth noting from this case.
First, if Hawker had hoped to cover his track through the use of a new alias (Dr. West), events soon proved him wrong. His alias cover fell apart quickly as within a few days, the arresting officer from Hawker’s 1871 case identified him as “Dr. Perry” from Emily Post’s death.
The second unusual element was the quiet dismissal of the Post case despite significant press coverage in February-March 1876. After May, the case disappeared from the press. I could find no subsequent references to the case that ever mentioned a trial or conviction. I can’t help wondering if Hawker’s allegedly healthy holdings in three different banks may have assisted him in discreet, behind the scenes fashion. The Philadelphia diploma mill criminal John Buchanan effectively deployed such a tactic to help legal paperwork disappear after greasing the palm of city clerks or aldermen. I suspect such possibilities existed in New York as well. The later 1895 NY Senate hearings under the Lexow Committee scandalized New York with its documentation of corruption (bribes, kickbacks) to police and others as a means of forestall scrutiny and arrests against physicians like Hawker providing illegal services. (Hawker appeared before the committee; his rival Newton Whitehead (see below) became a major witness)
As the various medical ads in the New York newspapers indicate, Benjamin Hawker had plenty of competition in drawing patients for his services. In 1877, Hawker fell into a protracted bitter rivalry with another physician, Dr. Newton Whitehead—an almost irrational rivalry whose end result saw Hawker convicted and sentenced in 1878 to a long prison term.
Excerpt1880 federal census. Dr. Hawker (mispelled as Erker) in prison in New York.
The bizarre series of reprisals between the two started in September 1877 when a disgruntled former patient of Hawker’s (Maggie McLoon) made her way to the office of Dr. Whitehead. She complained that Hawker relieved her of $50 (“all she had”) yet failed through his “operation” to terminate the pregnancy. Whatever the source of the enmity between the two men, Whitehead saw this as an opportunity to strike against Hawker. He escorted McLoon to an attorney promising she would “get justice.” The subsequent arrest of Hawker, Madame West and another associate led to the two doctors filing a series of legal complaints and counter-complaints with the courts. The headline of an October 3, 1877 news item summarized it best, “Doctors Quarreling.”
Matters only accelerated when Whitehead induced another Hawker patient, Amelia Hyde, to press charges related to an operation he performed on her. When Hyde failed to appear for the hearing, the case seemed dead–or so one would think. However, not yet content and eager to inflict his own blows against Whitehead, Hawker responded by filing a conspiracy charge of his own against Whitehead and Hyde. On the day of the hearing, Hawker went to court ready to support his conspiracy charge only to find that Ms. Hyde had shown up this time…and she was anxious to testify to Hawker’s medical malpractice.
The DA and judge resurrected the earlier dismissed case when Hyde failed to appear. This time Hawker’s luck ran out. Even the services of former New York mayor Oakley Hall, serving as Hawker’s attorney, couldn’t save him from a jury and press eager to see Hawker in the docket. Hawker played his last card—pressing charges with a resulting arrest of Dr. Whitehead—intended to keep his rival from testifying along with Hyde at his trial. All of this proved to no avail as the jury convicted him on March 1, 1878.
Former NY mayor Oakley Hall couldn’t save Hawker from prison
An unsympathetic judge sentenced Hawker, stating…:“Hawker, you have been convicted after a fair and impartial trial, upon an indictment for producing an abortion upon Amelia Hyde. You have been defended by one of the most famous lawyers in the country, but the jury convicted you. Upon that charge you are sentenced to be imprisoned in the King’s County Penitentiary for the term of ten years. That is all.”
Newspapers and social critics lauded the conviction. The Brooklyn Times Union congratulated District Attorney Isaac Catlin for producing the conviction, using almost precisely the same available evidence, that his predecessor Winchester Brinton had failed to secure. Anthony Comstock, leader of the New York Society for the Suppression of Vice, echoed the chorus lauding Catlin for securing a conviction.
In a letter published soon thereafter, Comstock told Catlin…“You started the ball in motion against this class of criminals, which, I trust, will not stop until every scoundrel in this damnable business of child murder gets his deserts. The public owe you and his Honor Judge Moore more than congratulations or thanks in this case.”
Anthony Comstock applauded Hawker’s conviction
Hawker and his attorneys filed various appeals—all of which failed. Hawker appears to have served the entirety of the ten-year sentence.
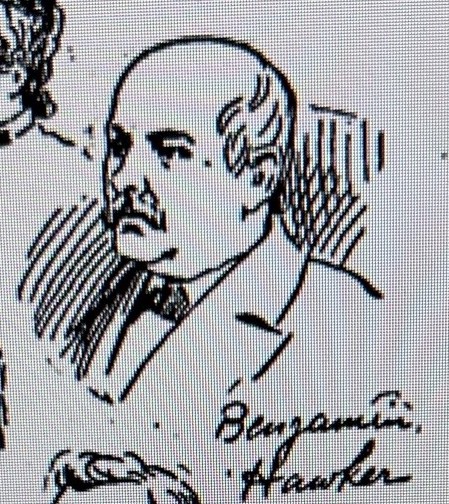
A decade spent in prison appears to have changed Hawker little—or perhaps he couldn’t envision any way to reinvent himself or make a living other than what he had by doing since 1870. In 1894, he and Whitehead were among the sixteen physicians, midwives and other self-styled doctors caught up in a police raid targeting medical “malpractitioners.” The assistance of an agent from the Society for the Enforcement of Criminal Law ensured major press coverage that included the New York World’s sketch artist presence at the chaotic court room scene. He quickly sketched the more infamous suspects, including Benjamin Hawker. This hastily drawn image is the only likeness of Hawker known to exist. Hawker posted $2,500 bail and disappeared.
Benjamin Hawker in 1894
Arrested two years later in 1896 for violating the state law barring felons from medical practice (described in my prior blog post), the legal path began that would take Hawker’s case all the way to the Supreme Court.
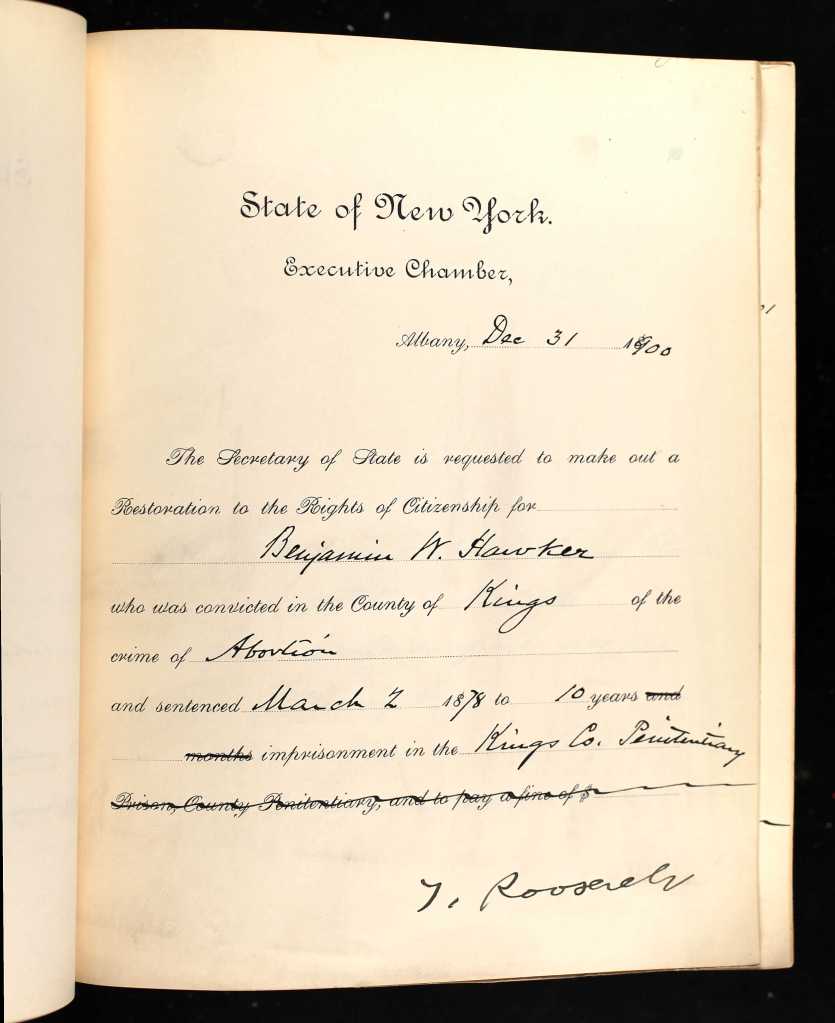
Hawker seems to have settled into a discreet medical practice in the aftermath of these legal decisions and effectively stayed off the radar of the authorities. He apparently supplemented his income by housing boarders at his home. His legal tribulations still weighed heavy with him as evidenced by his pursuit, and acquisition, of a commutation from New York whereby the state “restored [him]to all rights of a citizen.”
Excerpt from Hawker’s commutation with Gov. Teddy Roosevelt’s signature
In June 1903, Hawker reappeared in the news in shocking fashion–as the victim of a brutal assault that occurred from a botched home-invasion robbery.
Hawker survived a botched home invasion robbery
A former boarder, Dudley Bartlett, and his accomplice made plans to surprise, force him to open his safe and then chloroform him before making their escape. Little went according to plan as the accomplice bolted when Hawker and Bartlett engaged in a violent struggle for the gun. Repeated blows to the head and neck left Hawker badly injured and Bartlett apprehended.
Benjamin Hawker died at his home about six weeks later. The coroner attributed death to a diabetic coma, insisting—after consultation with Hawker’s treating physician, that the death was unrelated to the assault and injuries sustained six weeks earlier.
Hawker’s assailant was a former boarder who confessed all to the police
I’m torn as to what to make of Dr. Benjamin Hawker and his career. My curiosity about him stemmed simply from wanting to know the human story of the man behind a key Supreme Court case in the field of medical regulation. I wasn’t sure what I’d find in looking for him. I didn’t expect to find…well, I’ll just call him what many would—a career abortionist. Though I find myself loathe to condemn him with the sweeping moral assertions that some would impose.
Then again, perhaps nothing I found should surprise me. The lives of real people and their life trajectory rarely fit into tidy retrospective categories and labels. Life is messy; history is equally so.
The opinions expressed are those of the author and do not represent the views of the Federation of State Medical Boards.
Sources:
“The Brooklyn Abomination,” New York Daily Herald, August 31, 1871, p.6
“Medical Murder,” New York Tribune, September 2, 1871, p. 2
“The Courts,” Times Union (Brooklyn), September 23, 1871, p. 3
“The Courts,” New York Tribune, September 25, 1871, p, 2
“Medical,” New York Daily Herald, February 8, 1874, p. 16
“Dr. West,” Brooklyn Daily Eagle, March 3, 1876, p. 4
“Brecht Malpractice Case,” New York Times, March 5, 1876, p. 12
“Charged with Malpractice,” New York Times, September 20, 1877, p. 8
“Doctors Quarreling,” New York Times, October 3, 1877, p. 2
“Doctor Perry,” Times Union (Brooklyn), January 29, 1878, p. 4
“Another Chance for ‘Vindication’,” Times Union (Brooklyn), March 4, 1878
“The Courts,” Times Union (Brooklyn), March 6, 1878, p. 4
“Brooklyn,” New York Times, March 10, 1878, p. 2
“Charged with Malpractice,” Brooklyn Daily Eagle, March 24, 1894, p.12
“Held for Awful Crimes,” New York World, March 25, 1894, p. 13
“Physician Assaulted and Brutally Beaten,” New York Times, June 28, 1903, p. 2
“Physician was Careful,” New York Sun, August 3, 1903, p. 10
If you have been reading this blog or following me on Twitter (@davearlingtontx), you probably have a vague awareness of two U.S. Supreme Court cases critical to the evolution of medical regulation in this country. The earlier of the two cases, Dent v. WestVirginia (1889) is the better known thanks in large part to the scholarly work of James Mohr in Licensed to Practice (Johns Hopkins Press, 2013). Check out my May 2021 blog post for a refresher on Dent.https://armchairhistorian.blog/2021/05/
Less well-remembered and the subject of this blog post is Hawker v. New York (1898), a disciplinary case that complemented the Dent decision and its philosophic embrace of state licensing and regulation in medicine.
Hawker presents an intriguing case where the Constitutional prohibition against ex post facto laws (Article 1, Section 10) intersected with the Supreme Court’s doctrine of police powers exercised by the individual states, particularly in matters touching upon public health. I wrote about this important doctrine in a November 2017 blog post. https://armchairhistorian.blog/2017/11/
Hawker raised fundamental questions. For instance…
Are an individual’s actions from twenty years earlier evidence of their current moral character?
What if a reasonable requirement for current medical practice serves as an additional punishment for a past crime whose sentence has already been served?
What are the limits to the police powers of the state?
Dr. Benjamin Hawker had a troubled history as a medical practitioner in New York. His medical practice in the mid-1870s ran afoul on several occasions of the legal and cultural crusade against abortion led by Anthony Comstock and the New York Society for the Suppression of Vice. The key moment for Hawker (and this narrative) occurred in 1878 when the King County Court of Sessions convicted Hawker of criminal abortion and sentenced him to ten years in prison.
Fast forward nearly a decade. Now out of prison, Hawker returned to the practice of medicine in New York City, including continued provision of medical services placing him at odds with legal authorities and the court system. His arrest in September 1896 served as catalyst for a legal saga culminating in the Supreme Court’s decision in Hawker v. New York two years later.
At his 1896 trial, the New York City Court of General Sessions of the Peace convicted Hawker for violating Public Health Law (1895 rev., Sec. 153) which stated “any person who, after conviction of a felony, shall attempt to practice medicine, shall be guilty of a misdemeanor.” Hawker and his attorney appealed with a very specific legal argument in mind.
At the appellate court, the state presented the case as a simple matter—they pointed directly to Hawker’s 1878 felony conviction and section 153 of the 1895 public health law—i.e., Hawker had a prior felony conviction, defendant was caught practicing medicine; Hawker was guilty under New York law.
Hawker’s counsel argued that the law in question was written prospectively (i.e., with subsequent behavior in mind) and that the court erred by making a retroactive application of the 1895 law to an earlier (1878) felony conviction—an action they deemed ex post facto and thus, unconstitutional. In a February 1897 decision, the New York appellate court agreed with Hawker.
In reaching its decision, the appellate court acknowledged the right of the state to regulate the practice of medicine and, in doing so, to set conditions—both initial and new —as “necessity for them may arise.” However, the appellate court did not see this scope of authority as carte blanche for the state.
While the requirement under the law for “good moral character” was reasonable, the appellate court stated that this must relate to the “present status or condition” of the individual. The court held that by “seiz[ing] upon a past offense and mak[ing] that, and that alone…a new crime” the state of New York had overreached. The court further stated that the overarching intent of the law seemed designed to uniformly “deprive all convicted felons of the right of practicing at all.” Here it pointed to earlier U.S. Supreme Court decisions (Garland, Cumming v. Missouri) regarding legal restrictions aimed at former Confederate leaders.
Benjamin Hawker’s appellate court victory proved satisfying but short-lived.
The case then moved up to the NY Supreme Court a month later. In reversing the appellate court’s decision, the NY Supreme Court focused on three main points. The first involved another look at the 1895 New York Public Health Law. Hawker and his counsel had argued (successfully) that this law was written with prospective or future behavior as disqualifying, citing the language in Section 153. The NY Supreme Court disagreed, asserting that the language of that section must be read along with an earlier section (140) which set basic qualifications for medical practice. That section of the law stated: “…nor shall any person practice medicine who has ever been convicted of a felony….” [italics added] In pointing to that language, the NY Supreme Court ruled that the legislation had a specifically retrospective intent; that conviction of a felony, whether before or after 1895, disqualified an individual from practice of medicine.
The second major point identified by the court involved the assertion that the law was ex post facto and thus unconstitutional. Here the Court nimbly sidestepped the issue by pointing to Benjamin Hawker’s personal history. The court asserted “…it does not appear from the record…that he ever had any right to practice of the profession of medicine…and that no presumption can be indulged to that effect.” The Court claimed there was no evidence that Hawker ever studied medicine, obtained a medical diploma or even registered with the state to practice medicine. Thus, there was “entire absence of any evidence showing…he was deprived of any rights of property.” In other words, he wasn’t practicing legally, so there was no property right (i.e., his medical license) at stake. Think of this logic as “no harm, no foul.”
The final point addressed by the NY Supreme Court involved the doctrine of police powers articulated through a series of earlier U.S. Supreme Court decisions, i.e., the state’s authority to regulate the practice of medicine as a matter of public health. Here the Court sounded familiar notes on the unique role of the physician, necessary qualities of “trust and confidence” inherent to the nature of such practice, the legal precedent for states to impose “reasonable conditions and requirements” for practice, including good moral character. The court resolved the last point with the directness of Solomon—“the presumption of bad character attaches to a person convicted of a felony.”
While it is speculation on my part, I believe the NY Supreme Court’s sidestepping of the ex post facto element in the case is precisely why the US Supreme Court agreed to take up the case in 1898.
In a split decision, the U.S. Supreme Court sided with New York state. Justice David Brewer set forth the Court’s reasoning in its decision.
Supreme Court Justice David Brewer
He began by acknowledging the “single question” presented by the case—the constitutionality of New York’s law relative to the U.S. Constitution’s prohibition against ex post facto laws. Brewer began with a recitation of the Court’s thought processes from a decade earlier in Dent v. West Virginia. To wit: The state’s acknowledged authority under the police powers doctrine to “prescribe…qualifications” for any individual or business impacting the health of the public; the reasonableness of qualifications calling for both knowledge and good character; and that the state can “make the record of a conviction conclusive evidence of…absence of the requisite good character.” Brewer conceded that “no precise limits have been placed upon the police power of a state”; signaling that such limits might yet be clarified in subsequent case law.
Brewer continued by pointing to multiple state court decisions affirming the state’s right to include good moral character as a reasonable condition for the regulation of medical practice—specifically, the state’s authority to identify or determine “evidences” of what constituted good moral character. Thus, if a state such as New York determined that conviction of a crime precludes current or future practice of medicine, they are simply exercising res judicata, not imposing an unreasonable additional punishment. In essence, the majority opinion proved willing to grant the state a wide latitude under the police powers doctrine; showing strong sympathy for the broad concerns for public health set forth earlier in Dent. These considerations carried the day.
Interestingly, Justice John Marshall Harlan’s dissenting opinion focused almost exclusively on the issue of the ex post facto nature of the legislation. He argued that Hawker’s attorney had been correct in pointing to the precedents set by the Court in the Garland and Cummings cases. In those cases, the Court showed a zealous protection of fundamental rights (life, liberty, pursuit of happiness), even for individuals once in open rebellion against this country. To wit: “exclusion from any of the professions…for past conduct can be regarded in no other light than as punishment for past conduct” and “any deprivation or suspension of any of these rights for past conduct is punishment.”
Supreme Court Justice John Marshall Harlan
Reading the text of the Hawker decision today, what I find most striking is the deference and wide latitude offered to an emerging medical profession. I don’t believe this deference was a given at the time the Hawker and Dent cases reached the Court. We can look back at these cases today and see medicine poised for, and on the journey toward, what it would later become—the modern wonder that we see when we think of it now. The Court enjoyed no such prescience.
Here it is important to keep in mind the state of medicine at the time of the Hawker decision. While the late 19th century witnessed major leaps forward in medical knowledge, there remained a distinct gap (chasm is more apt) when compared with advances in therapeutic treatment that lagged far behind. In essence, the medical profession had a far greater understanding of the mechanisms underlying disease and illness than its ability to effectively treat or eradicate many of them. This efficacy was still years away. So why did the Court side with New York state (and thus, the medical profession) rather than the Constitutional prohibition against ex post facto legislation?
I believe the answer rests with an assumption…one described by historian James Mohr. The degree to which the Supreme Court in Hawker and Dent placed medicine in a privileged social and legal position speaks predominantly to unspoken assumptions—that medicine and its practitioners had successfully transformed itself from vocation to profession; that a specialized body of knowledge existed that warranted, even demanded, close monitoring of those practicing medicine; that medical progress would continue on a path benefiting patients and public health in general. Perhaps not as fully or effectively in 1898 as one might desire but one sure to fulfill its promise in the years to come.
And Benjamin Hawker? Well…there’s a good deal more to share about this otherwise long-forgotten physician beyond the attachment of his name to an important Supreme Court case. Check back for my next post when I share the surprising things I learned about Hawker.
The opinions expressed are those of the author and do not represent the views of the Federation of State Medical Boards.
Sources:
William H. Silvernail, The New York Criminal Reports: Reports of Cases Decided in all Courts of the State of New York (Albany: W C Little & Co., Law Publishers), 1898
Marcus T Hun, Reporter, Reports of Cases Heard and Determined by the Appellate Division of the Supreme Court of State of New York (Albany: Banks & Brothers) 1897
Stephen K. Williams, LL.D., Cases Argued and Decided in the Supreme Court of the United States, 167, 168, 169, 170 US. Book 42 Lawyer’s Edition. (Rochester: Lawyers Co-operative Publishing Co., 1920)
Ask anyone who has conducted historical research and they’ll likely offer their own example of the scenario I’m about to share. You’re deep into researching one thing when suddenly you run across something entirely unexpected, only to find yourself irresistibly drawn away from what you were initially researching. Think dog sees squirrel and you’ll get the picture.
You feel exhilarated tracking a little-known subject or story that seems to offer intriguing possibilities; you also can’t help feeling irritated with yourself for losing focus and valuable time traipsing deeper into a research forest well-off the main trail.
In this instance, my research subject was Dr. Benjamin Hawker, the litigant in the key Supreme Court decision Hawker v. New York that secured the authority of state medical boards to discipline physicians. My attempts to trace Hawker’s backstory led to some extensive online research. Somewhere along the way, I stumbled upon “Dr.” Edward Dowdall. His story offers a reminder of the white-collar criminal elements that gravitated toward medicine in the late 19th and early 20th centuries. The persistent activities of Dowdall and his ilk created a good deal of additional work for state medical boards.
In spring 1906, Dr. Seymour Doss (S.D.) Van Meter, Secretary of the Colorado Board of Medical Examiners (pictured below) received an odd letter from an Illinois physician requesting a “favor.” Edward Dowdall explained that he wanted to obtain a Colorado medical license but didn’t feel “overconfident” the board would accept his application.
Furthermore, he wanted a Colorado license even though he didn’t wish to practice in the state. He confessed that there were so many doctors in the state that “I fear I would starve to death in Colorado.” Still, if Van Meter would “help me out” he (Dowdall) would return the favor with a gold watch and a diamond set locket.
Van Meter must have been surprised by the clumsy but direct bribe offer for a license he didn’t intend to use. In closing the letter, Dowdall made clear his ultimate objective—he wanted to practice in New York state. His plan was to get the Colorado license and bide his time (“lay dormant” for a few years as he described it) before using that Colorado license to get licensed in New York.
Dr. Van Meter joined the Colorado board in 1901. Over the subsequent twenty years of his service on the board, he enjoyed a front-row seat to many attempts to circumvent the regulatory system. In a delightful 1925 article, “Medical Forgeries,” Van Meter shared stories of the fakes, frauds and imposters that he and the board encountered. Dowdall’s awkward attempt at bribery—while striking in its directness—lacked sufficient deviousness to make the cut for inclusion in Van Meter’s1925 reminiscence piece, but he knew already how to handle such matters.
He responded to Dowdall with an “encouraging” letter and asked for two photos. Dowdall responded with the requested photos and information, intended (so he assumed) for his Colorado license application. Instead, Van Meter forwarded all their correspondence to Dr. James Eagan, Secretary for the Illinois Board of Health.
As it turned out, Eagan and colleagues were already investigating Dr. Dowdall for several misdeeds in that state. Practicing medical without a license was one infraction. The one that authorities seemed most focused on involved allegations that Dowdall attempted to secure money under false pretenses—specifically, securing hundreds of dollars from medical students and prospective midwives by promising he could “fix” things with the Illinois Board through a “charitable scrutiny” in scoring their licensing examination.
The case against Dowdall only grew stronger when the arresting authorities found bogus diplomas from the American Association of Physicians and Surgeons. Dowdall had apparently sold a large quantity of these for as little as $5 each.
What also came out at that time was the reason why Dowdall felt he couldn’t legitimately secure a license from the Colorado board: while practicing medicine in Detroit he had been sentenced in to 7 years for perjury in a botched effort by Dowdall and a female companion to punish a rival physician through a sexual assault claim. Dowdall sat in prison from 1899 until sometime prior to July 1905.
He apparently arrived in the Chicago area after Port Huron, Michigan police “ordered [him] to leave the city” in 1905. He was practicing medicine without a license in Illinois when Eagan received the bundle of letters from Van Meter.
A Chicago jury convicted Dowdall in August 1907 but from there the paper trail disappears entirely. We don’t know what sentence the court imposed. We don’t know whether Dowdall lingered in the area afterward or made his way east to ply his trade (medicine? Fraud?) in New York City.
Dowdall presents a good example of the weaknesses of the medical regulatory system of that era. Take the matter of his medical credentials. In 1890s Michigan, the basis for a medical license was a diploma from a “legally chartered” institution. Don’t be fooled, however, by the gravitas suggested by the term, “legally chartered.” This represented a low standard as laws governing the issuance of school charters were notoriously lax in many states. A medical degree from a “legally chartered” medical school was easily obtained as Dowdall knew first-hand. While he claimed to have graduated from Trinity College (Dublin), the specific degree he presented for licensure was from the Independent Medical College of Chicago—a fraudulent school notorious as a medical diploma mill. (The Illinois Supreme Court revoked the school’s charter in 1899.)
Another weakness was the anemic statutory language in many states for regulating medical practice in those days. When Dowdall was convicted of perjury in 1899, only nineteen states gave their medical board the authority to revoke a license they had previously issued. Michigan was among the nineteen. So even though Dowdall had a perjury conviction, the Michigan board could not remove his license to practice…though local authorities apparently found ways to make life sufficiently uncomfortable that he opted to leave for Chicago.
Another weakness stemmed from the poor communication among and between medical boards. This was precisely the flaw that Dowdall intended to exploit with his clumsy attempt at a Colorado license. He knew that his Michigan license was tainted by his perjury conviction in that state. Thus, he needed a clean license as the basis for trying to secure a license in New York without having to reference his time in Michigan. If Dowdall could’ve obtained that Colorado license and laid low for a few years, his application for a New York license ca. 1908 or so would’ve been based upon that Colorado license and passing the New York licensing exam. If he could pass the exam (no small hurdle) he would’ve been open for business in the relative anonymity of New York City’s metropolis.
Looking back at this era, we can see this sprinkling of non-violent, white collar criminal types hovering around the fringes of medical licensure and practice. I don’t believe there were necessarily a lot of these types but just enough to require regulatory vigilance. I guess we shouldn’t be surprised. Once a license became mandatory in order to legally practice medicine, both the medical degree and the license itself acquired an economic value as credentials and as the basis for income beyond that of the average worker.
As for Benjamin Hawker? Dowdall only sidetracked me so long. I’ll write about Hawker v. New York and the good doctor’s surprising backstory in my next posts.
The opinions expressed are those of the author and do not represent the views of the Federation of State Medical Boards.
It would be naïve to think that this nation’s fraught history with race did not impact medical regulation. The challenge here, as for all the categories explored in this post, is pulling together a reasonable overarching narrative from fifty different states. If we pull back to a thirty-thousand foot view for medical regulation, however, there was one development that carried by far the greatest impact.
Black Americans faced limited opportunities for medical education and, ultimately, licensure in the late 19th and early 20th century. These opportunities were curtailed further by reform measures in medical education such as those by the Carnegie Foundation and the AMA Council on Medical Education. While the Carnegie Foundation’s Flexner Report remains the better known of these efforts, the Council on Medical Education’s inspection and rating system for U.S. medical schools proved even more impactful. You may wonder, “How is this relevant to medical regulation?” I’ll explain.
The Council created a 3-tier rating system that categorized all schools as Class A, Class B or Class C. The first two categories either met standards or were deemed capable of doing so with reasonable changes. Class C schools were classified as substandard and deemed unsalvageable. This categorization system carried a profoundly negative impact to historically black medical colleges (HBMCs), nearly all of which fell into the Class C grouping.
With the exception of Howard, HBMCs were proprietary endeavors chronically short on funding and resources. Yet they were often the only option available to black physician hopefuls. As state legislatures and medical boards –desirous of higher standards for medical education and plagued by persistent diploma mill style educational endeavors—eagerly embraced the Council’s rating system. The classification system fit conveniently and without ambiguity into state law and seemed a mom-n-apple pie recipe for improving the quality of this nation’s physicians.
The downside? Once this became a primary basis for licensure, HBMCs routinely found themselves assigned to the Class C category with their graduates’ ineligible for licensure in all but a few states by 1923. This reality contributed to a death spiral for all but two HBMCs (Howard, Meharry) and represented a massive setback for black Americans aspiring to become licensed physicians.
Leonard Medical School in Raleigh, North Carolina was the most prominent HBMC to close in the wake of states’ adoption of the AMA Council’s classification system for medical schools
While this systemic factor cannot be emphasized too much, there was also impactful activity happening around licensing decisions specific to individual physicians. Here it is difficult to generalize without succumbing to speculation. So I will offer a few anecdotes though I acknowledge that the plural of anecdote is not evidence!
Justina Ford was the first black female physician licensed in Colorado. The year was 1902. Her encounter with the Colorado board left an indelible memory. As she related the story later, one board member told her: “I’d feel dishonest taking a [licensing] fee from you. You’ve got two strikes against you. First off, you’re a lady and second, you’re colored.” Her low-key response suggested she would be a persistent licensure applicant. “I know it. I thought it all through before I came. This is just the place I want to practice.”
Justina Ford, MD
Or take the example of the North Carolina Medical Board. For roughly 40 years, the Board’s administrative practice was to annotate the record of black licensure applicants with a “col” or “colored.” I wrote about this practice recently in the North Carolina Historical Review though the extant evidence and data available were ambiguous as to whether this impacted the scoring of their examination.
Note the “col” annotation for Drs. Pope, Scroggins, Williams.
It seems highly unlikely that North Carolina was the only state medical board utilizing this annotation practice. It was common to see state medical journals and JAMA publishing updates from medical boards on the administration of their licensing exam…and also common for these narrative pieces to call out the number and/or performance of “colored” candidates. Clearly, someone at these boards was keeping track; and in an era when extended response/essay questions were the norm…well, scoring these licensing exam questions was inherently a subjective matter by the board member(s). Scorer bias—whether racial or subject-matter specific—was impossible to remove from such a testing format.
The Journal of the National Medical Association commented in 1910 on the challenge confronting black physicians to receive due and appropriate credit for their performance on state licensing examinations. Historian Neil McMillian asserted that it was “an article of faith” among black physician candidates in Mississippi that prejudice impacted licensing decisions in that state. The truth behind these concerns and perceptions—to the extent it is recoverable at all—is buried in records dispersed across fifty states. Records that may be suggestive but not explicit about this reality.
Final thoughts
I know that some readers will react to a blog entry like this and think I’m picking at an old wound…that I’m focusing unnecessarily on past shortcomings rather than celebrating the more recent successes in the regulatory narrative. I guess that is one way to interpret this post.
I would hope, however, that readers of this blog over the past few years will see this piece for what I intended—to share what I suspect is a lesser-known aspect of the history of medical regulation; to tell stories—both good and bad—about this unique field; and to inform today’s regulators about the rich history in their field as helpful context for the important work they do today.
Select sources:
Federation Bulletin spanning multiple years from 1915-1926.
“State Board Statistics” in JAMA. This extensive presentation of aggregated information/data appeared annually in April-May.
Marilyn Griggs Riley, High Altitude Attitudes: Six Savvy Colorado Women (Boulder: Johnson Books, 2006)
David Alan Johnson, “The North Carolina Medical Licensing Examination, 1886-1925: Analysis of Performance by Examinees from Historically Black Medical Colleges,” The North Carolina Historical Review (April 2021).
The opinions expressed are those of the author and do not represent the views of his employer (Federation of State Medical Boards)