“An institution is the lengthened shadow of one man.” Ralph Waldo Emerson, Self-Reliance, 1841
I remember coming across this quote many years ago and being struck by its pithy expression of a profound truth. One that many of us do not fully appreciate until later in life—when our own experiences and accumulated years bring an understanding that the vagaries of human existence make it all the more remarkable when any company, organization or institution manages to survive beyond a few decades. Longevity stands out in a world littered with Kodaks, Sears planned obsolescence and unanticipated technical disruption.
Approaching retirement from the Federation of State Medical Boards (FSMB), I cannot help but reflect on the trajectory of my career and the organization that did so much to foster it. Nearly 29 years with the FSMB has offered a life lesson in the ebbs and flows that are a natural part of the life cycle of any long-standing organization. I’ve seen leadership navigate challenges large and small over nearly three decades. Success—both immediate and long-term—is seldom accidental, but the result of a clear vision, steady temperament and a dash of good luck along the way.
I share this because my knowledge of the history of FSMB and medical regulation in this country underscores that some institutions emerge from specific circumstances and survive—as Emerson suggests—due largely to the contributions of a single individual. This blog post represents the first in a series spotlighting the impact of several individuals who proved instrumental to the history and development of medical regulation in this country.
Walter Bierring, MD (1868-1961)
Let me start by saying that I and all my FSMB colleagues should thank Walter Bierring for our jobs. It is not an overstatement to say that if not for him, the FSMB probably would not exist today.
An intellectually curious and ambitious son of Danish immigrants, Bierring attended medical school at the University of Iowa and later pursued training in Europe: Heidelberg (1892), Vienna (1896), Paris (1901). Bierring worked as a medical educator (Univ. of Iowa; Drake) until 1913 when his focus shifted toward professional and regulatory interests. His addition to Iowa Board of Health and later the state medical board brought him directly into the orbit of the FSMB.
Bierring’s talents and leadership were quickly recognized. In 1916, FSMB President Charles Cook wrote Bierring to confide his belief that the latter was key to the organization’s ultimate success.
“The future of the Federation, as I see it, is today largely in your hands…you know its past history, the pitfalls to be avoided, the problems to be solved, lines of work to be taken up, the danger of its being over-shadowed by other organizations….”
Cook’s prophecy held true. Bierring served as the FSMB Secretary-Treasurer from 1915-1960 and as the editor of the Federation Bulletin during nearly all of that span of time.
Why was Bierring so integral to the FSMB’s success and survival? It’s simple. He served as the key player sustaining the organization at a time when it had no full-time paid staff, no permanent national offices, no specific product/service generating revenue and minimal resources derived from modest membership dues and in-kind resource assistance from the AMA. For more than 45 years the “work” of FSMB was largely sustained by this one man from his home in Iowa. Bierring carried the FSMB through its most trying times in the 1930s and early 40’s. For all intents and purposes, Bierring was the Federation during the organization’s leanest years.
Looking back, it is easy to see that the organization might have slipped into a moribund condition and total irrelevance. Indeed, it might well have collapsed entirely without him. Knowing the FSMB today, this seems unimaginable and yet such an outcome was clearly possible, and ultimately avoided, due largely to Bierring’s contributions and steady hand over four decades.
So how did he do it? Patience, dogged persistence and force of personality. Bierring’s leadership style mirrored the attributes identified by business writers as critical to successful CEOs: humility, curiosity, a collaborative-spirit. Despite the accolades that came his way, Bierring shared credit freely with his colleagues. Over the years he wrote a series of articles highlighting the contributions of other FSMB colleagues. Bierring preferred winning over opponents through reasoned conversation and a bit of charm. As one of his contemporaries described him, Bierring was “always constructive, never destructive.” He preferred quiet diplomacy to direct confrontation—what today we call consensus-building.
When necessity arose, he could be forceful in his own way—particularly in exerting influence. One contemporary described his approach as an “iron fist in a velvet glove.”
Bierring didn’t innovate a product or service; he didn’t blaze new trails on the policy or legislative front. What he understood best was people and how to work with and through them for a desired goal—and at the right pace. For the leader of any membership organization this is a critical skillset. Operating in such a way that you are neither too far in front nor so far behind that you risk losing those you are seeking to lead.
Walter Bierring represented the longest single strand of continuity linking the organizations from its earliest days to the cusp of its resurgence in the early 1960s into the modern organization that exists today. If not for Walter Bierring, it’s unlikely the FSMB would have survived long enough to enjoy that reemergence.
Perhaps a former FSMB President said it best: “…the most fitting and lasting tributes to Dr. Bierring is the Federation itself. This is his true testimonial…he has laid the foundation and it is up to us to build and carry on.
Thank you, Dr. Bierring.
The opinions expressed are those of the author and do not represent the views of the Federation of State Medical Boards.
Source:
This blog post is adapted from chapter 5 of Medical Licensing and Discipline in America: A History of the Federation of State Medical Boards (2012)
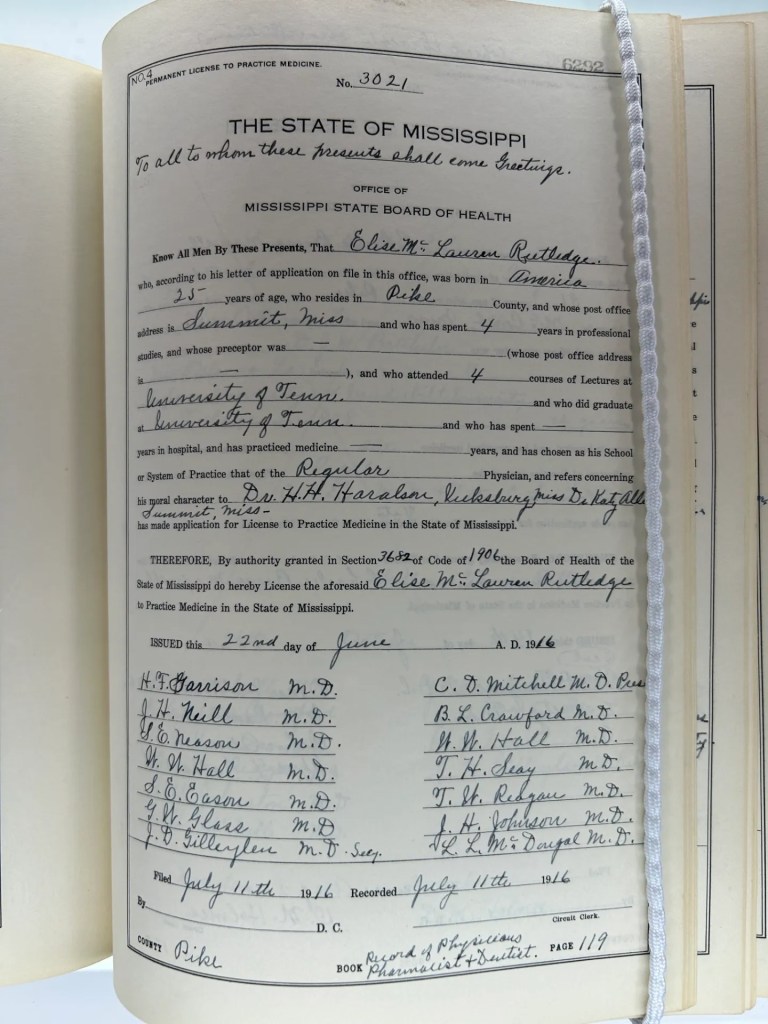
I’ve written before about the donated materials contributed by the Mississippi Board of Medical Licensure to the FSMB Historical Collection (FHC). https://armchairhistorian.blog/2025/10/07/preserving-the-history-of-medical-regulation/ Among the donated materials are a two-volume set containing all the questions (organized by year and subject area) presented to candidates on that state’s medical licensing exam between 1924-1958.
This gift piqued my interest as well as that of a colleague. As we considered the source materials donated to the FHC, various ideas and questions came to mind: How challenging were these state-developed medical licensing exams? Were they quality exams requiring candidates to apply relevant medical knowledge? Or were they exercises in recall too often seeking factoids or obscure medical trivia? There was a lot riding on the outcome of these exams—a medical license, a career and professional livelihood. So were these exams constructed, administered and scored in a manner commensurate with the high-stakes nature involved with the licensed practice of medicine?
We undertook something akin to a case study of the Mississippi licensing exam, blending two approaches: (1) AI and human rater analysis of these the Mississippi test questions, and (2) review of performance data on the Mississippi exam. My next blog post will share some of what we learned about the former. Today, I want to focus on this latter, starting with how these exams were constructed.
Structure and format of the Mississippi exam
From its originating legislation in 1882, Mississippi required physicians to pass a written examination conducted by its examining body. (Note: There was an exemption in this original law that allowed established practitioners in the state to forego the exam).
A ten member Mississippi Board of Health wrote and administered their state’s licensing exam. The twelve subject areas covered on the exam during the 1924=1958 period are listed here.
Anatomy* Physiology* Hygiene* Obstetrics* and Gynecology Surgery* Pathology* Histology/Bacteriology Chemistry* Diseases of eye, ear, nose, throat Materia Medica* Theory and Practice of Medicine Physical Diagnosis
*indicates original subject areas called for in the 1882 legislation
Individual members of the Mississippi Board wrote six to ten questions for their assigned subject area. All questions were constructed as “open” or extended response items. There were no multiple-choice questions (MCQs) on the Mississippi exam during this period. This is hardly surprising. MCQs did not feature prominently on any state exams for medical licensure or on the National Board of Medical Examiners Parts exam until the 1950s.
Absent information to the contrary, it is presumed that the board member writing the questions for a subject area also carried the responsibility for scoring those items.
I have found no detailed information on the scoring scales or requirements specific to achieving an overall passing level performance on this exam. The 1882 law called only for candidates to present an examination that “prove[d] satisfactory” to the Board.1 As late as 1947, the law only referred to the examination results providing evidence of “sufficient learning.”2 The various volumes donated by the Mississippi board to the FHC do not present any specific information on the scoring. Thus, we don’t know the answer to a few basic questions: Did the Board require a passing score on each individual subject area in order to achieve an overall passing outcome? Or were subject area scores rolled up into an aggregate score with its own specified minimum for passing? (Note: States commonly specified 75 in their state statute as the minimum pass.)
Exam performance data
So how tough was this Mississippi exam? To answer this question, I leveraged the data collected and published annually in JAMA as “State Board Statistics” (1924-1929) and subsequently retitled as “Medical Licensure Statistics” (1930-1958).
For the 35-year period spanning the years 1924-1958, a grand total of 1,768 individuals were examined by the Mississippi Board—an average of 50 candidates per year. And the results? We are definitely not talking about the Bataan death march of assessment. All but 23 candidates passed the exam—a 1.3% fail rate for this entire period! (See the Appendix 1 below)
From a purely statistical perspective, this exam presented a minor hurdle for the vast majority of candidates. Indeed, in twenty-three of the 35 years of this study no candidates failed the exam in Mississippi. Though this may seem surprising it was actually not uncommon based upon the reported performance outcomes on other states’ medical licensing exams. Looking nationally at the period 1924-1958, twenty-three states reported years in which no candidates failed their medical licensing exam. Thus, Mississippi’s modest 1.3% overall fail rate ranks 25th (median) among all states during this period. (see Appendix 2)
Interestingly, this was definitely not the case previously on the Mississippi exam. Only a decade earlier, the fail rate on Mississippi’s exam fell on the other end of the spectrum. The first 5-year period reported by JAMA showed Mississippi with the highest failure rate on its exam compared to all other states.
Years
# MS candidates
% failed
National rank
1908-1912
1,172
55%
1st
1914-1918
284
23%
11th
1919-1924
124
8%
25th
A dramatic swing involving the Mississippi exam took place sometime around the start of World War I. What happened precisely is unclear but we can speculate on reasons for both the sharp drop-off in number of candidates being examined by Mississippi after 1912 as well as the steady decline in their fail rate.
In terms of the volume drop off, prospective licensees may have begun avoiding Mississippi because of the high fail rate on its exam which would have been publicly known through JAMA’s annual publication of state specific exam results. It is also possible that changes to state law or board policy may have directed more incoming physicians from other jurisdictions into licensure by reciprocity or endorsement scenarios that allowed them to bypass the exam. Perhaps the strongest factor in the declining numbers and also the fail rate was the change to state law in 1919 that required licensure candidates to be graduates of Class A school2 under the AMA Council on Medical Education’s classification system.
It also bears mention that Mississippi had one of the lowest physician-to-population ratios in the United States at 1:1640. Board Chair Felix Underwood called it the “most serious and complex public health problem” in the state’s history.3 With the Mississippi Board keenly aware of this shortage, I can’t help but wonder if this worked at least unconsciously on the Board’s vetting of physician candidates and even its scoring of candidates’ exams. See Appendix 3
By 1914 and through the start of World War II, the number of physician candidates examined by the Board stabilized at a modest twenty to thirty annually in most years with a fail rate hovering around 2%.
Mississippi board composition and impact on the exam
The ten-member Mississippi board wrote and administered its medical licensing examination. Board members served six-year staggered terms. Assuming scoring was done by a single board member for each subject area, changes to board composition directly impacted both the exam’s content and its scoring.
Thirty-five (35) individuals served on the Mississippi board during the period 1924 to 1958. The mean length of service was nearly a decade (9.57 years) with a dozen individuals serving 12 or more years on the MS board. Board Secretary Felix Underwood served 34 years, nearly the entire span of the time period under review. See Appendix 1
Paying attention to the Board’s composition is more than just historical minutiae. With an extended-response item format, the individuals making decisions about the correctness and sufficiency of the answers (i.e., the rater) represents the key factor impacting scoring and overall pass rates on the Mississippi exam. The information available to us does allow for analysis concerning how the number of raters scoring each subject area impacted potential scoring (in)consistency.
While two subject areas (Histology/Bacteriology and OB/GYN) had higher potential consistency by virtue of the small number of board members scoring those areas during this period, most subject areas had 3-4 different board members scoring that component of the exam from 1924-1958. Two areas (surgery, EENT) had probably the greatest potential for scoring variability.
Subject area
# scorers
Subject area
# scorers
Histology/Bacteriology
1
Pathology
4
OB/GYN
2
Physical Diagnosis
4
Anatomy
3
Theory & practice of medicine
4
Hygiene
3
Materia Medica
5
Physiology
4
Surgery
7
Chemistry
4
Diseases of eye, ear, nose, throat
7
We might think that a single examiner scoring a subject area over the entire period is the ideal. While such was the case for histology/ bacteriology, the practical reality is that the time-period in question is so long that there were likely multiple changes over time impacting the judgment of a sole rater on an biannual test administration. For instance, rater tendencies and predilections involving specific focus or emphasis in crafting questions within the subject area; changing expectations of what constitutes an acceptable minimum level of performance by a candidate, etc. In other words, how a rater approached both what questions to ask and how they should be scored ultimately shift over time even when only a single rater was involved in a subject area. As one scholar put it, “assigning a grade to an essay is not a precise science.”4 This is not conjecture. Ample evidence exists in the scholarly and technical literature specific to scoring extended response items demonstrating that rater (in)consistency is highly problematic to exam reliability.
At the same time, it seems unlikely that the rater composition, regardless of (in)stability, had much impact on licensure candidates in Mississippi. Why? Going back to the performance data, few individuals (n=23) failed to demonstrate adequate knowledge to that board. The examination in Mississippi presented an easily surmounted hurdle in the candidate’s journey to licensure.
So was the medical licensing exam in Mississippi little more than pro forma ritual? A performative exercise for gaining admittance to the profession? Perhaps. But in order to answer this we have to look directly at the questions being posed on the Mississippi examination. How relevant were they? Were they quality items allowing the rater to glean insights into the knowledge and competence of these candidates? For this, we sought subject matter review. That will be subject of my next blog post.
To be continued….
The opinions expressed are those of the author and do not represent the views of the Federation of State Medical Boards.
Endnotes
See Section 17 of An Act to Regulate the Practice of Medicine in the State of Mississippi (Jackson: State Printer, 1882).
Mississippi Laws and Extracts of Laws Dealing with Public Health (Jackson: Mississippi State Board of Health, 1947), 104
Lucie Robertson Bridgforth, “Politics of Public Health Reform,” The Public Historian, 1984, p. 19
Gavin T. L. Brown, “The Reliability of Essay Scores: The Necessity of Rubrics and Moderation,” in Tertiary Assessment and Higher Education Student Outcomes: Policy, Practice and Research. Ed. Luanna H. Meyer, et. al. 2009
Appendix 1
All candidates for Mississippi examination
Year
Total
# pass
# fail
Fail %
MS fail % compared to nat’l
# states w/ 0% fail
1924
21
20
1
4.7%
21st
28
1925
28
28
0
0%
24th
27
1926
20
18
2
10%
5th
25
1927
21
21
0
0%
35th
16
1928
24
24
0
0%
32nd
19
1929
27
27
0
0%
30th
21
1930
33
31
2
6.0%
10th
27
1931
35
35
0
0%
25th
26
1932
27
27
0
0%
25th
26
1933
24
24
0
0%
26th
25
1934
29
28
1
3.4%
14th
22
1935
31
30
1
3.2%
16th
19
1936
26
22
4
15.3%
8th
26
1937
18
22
2
9.0%
14th
18
1938
32
31
1
3.1%
16th
21
1939
22
22
0
0%
25th
26
1940
42
42
0
0%
28th
23
1941
38
38
0
0%
27th
24
1942
45
43
2
4.4%
14th
24
1943
114
113
1
0.9%
23rd
22
1944
60
60
0
0%
24th
27
1945
50
50
0
0%
25th
26
1946
45
45
0
0%
28th
23
1947
59
59
0
0%
22nd
29
1948
47
47
0
0%
27th
24
1949
40
35
5
12.5%
7th
19
1950
64
63
1
1.5%
22nd
21
1951
77
77
0
0%
28th
23
1952
83
83
0
0%
27th
24
1953
84
84
0
0%
25th
26
1954
80
80
0
0%
27th
24
1955
75
75
0
0%
33rd
18
1956
101
101
0
0%
32nd
19
1957
122
122
0
0%
34th
17
1958
124
124
0
0%
26th
25
Total
1,768
1,745
23
1.30%
Mean 20th
Mean 23
Median 25th
Median 24
Mode 25th
Mode 26
Source: Compiled from JAMA “State Board Statistics” (1924-1929) and “Medical Licensure Statistics” (1930-1958). This appeared annually—usually in April or May.
Appendix 2
# of Physicians in MS, 1938-1947
Year
Total
White
“Colored”
1938
1446
1392
54
1939
1436
1381
55
1940
1425
1372
53
1941
1356
1306
50
1942
1330
1279
51
1943
1200
1151
49
1944
1160
1111
49
1945
1112
1060
52
1946
1213
1163
50
1947
1351
1298
53
319 MS physicians served in WWII
Source: Public Health and Medical Licensure in Mississippi, Vol 2. FJ Underwood, RN Whitfield. Jackson: Tucker Printing House, 1938, p. 378
Appendix 3
Mississippi Board members 1924-1958
Board member
Years serving
Total # Yrs
Subject area
Arrington
1958
1
pathology
Austin
1924-1943
20
Anatomy; Materia medica
Avent
1947-1958
12
Chemistry
Banks
1934-1957
24
Pathology
Blackburn
1950-1958
9
Hygiene
Brock
1936-1941
6
Physiology
Brown
1925
1
Material medica
Caldwell
1944-1958
15
EENT; Surgery
Crawford
1926-1929
4
Surgery
Culpepper
1942-1947
6
Physical diagnosis
Dampeer
1924-1929
6
Physiology
Darrington
1931-1935
5
Surgery
Dearman
1931-1935
5
Physical diagnosis
Eason
1924-1951
18
OBGYN
Field
1942-1958
17
Physiology; Materia medica
Frizell
1930-1935
6
Physiology
Gamble
1944-1956
13
Anatomy
Garrison
1948-1958
11
Theory, practice of medicine
Gavin
1924-1925`
2
Hygiene
Haralson
1924-1925
2
Pathology
Holmes
1925-1927
3
Chemistry
Hooper
1924
1
Chemistry
House
1952-1958
7
OBGYN
Howell
1936-1941
6
Surgery
Lipscomb
1926-1943
18
Theory, practice of medicine
Long
1942-1948
7
Surgery
McKinnon
1936-1941, 1948-1958
17
EENT, Physical diagnosis
Seale
1925
1
Theory practice of medicine
Shaw
1928-1946
19
Stennis
1926-1933
7
Pathology
Underwood
1925-1958
34
Histology/bacteriology
Wall
1924-1925
2
Surgery
Watson
1926-1929
4
EENT
Wilkins
1957-1958
2
Anatomy
Wright
1926-1949
24
Hygiene
35 members
Average length of service in years: Mean 9.57 Median 6 Mode 6
Source: Two-volume set of Mississippi Board of Health licensing exam questions housed at the FSMB Historical Collection